

Most healthcare professionals will tell you they learn from experience. Unexamined experience does not reliably produce learning, though. It produces habit. Reflective practice is the process that turns experience into insight, and insight into better clinical behaviour. This post covers what the research shows, how the main frameworks work, and how to build reflective practice into clinical training systematically.
What Is Reflective Practice in Healthcare?
Reflective practice is the deliberate examination of your own actions, decisions, and responses, with the aim of improving future performance. It is not the same as thinking back on what happened. Donald Schön, whose work laid the theoretical foundation, described two modes: reflection-in-action, where a practitioner adjusts their approach while an interaction is still unfolding, and reflection-on-action, where they examine what occurred after the fact to draw conclusions (Schön, 1987). Both are active processes. Both require the practitioner to interrogate their choices, not merely recall them.
Sandars’ AMEE Guide No. 44 identifies metacognition, the capacity to monitor and regulate your own thinking, as the core mechanism through which reflection operates (Sandars, 2009). This framing matters for training design: if reflection is a metacognitive skill, it can be taught, scaffolded, and assessed. It is not an innate tendency that some practitioners have and others lack.
In healthcare, this matters because clinical encounters are too complex and fast-moving for full conscious attention in the moment. A trainee delivering a difficult diagnosis cannot simultaneously perform the conversation and evaluate how they are performing it. Reflection closes that gap retrospectively, converting lived experience into transferable knowledge.
What the Research Shows
The evidence base for reflective practice in healthcare education is consistent across settings and disciplines. A systematic review published in Advances in Health Sciences Education analysed reflection across health professions education and found repeated associations with improved clinical judgment, professional identity development, and emotional resilience (Mann, Gordon & MacLeod, 2009). The review identified that reflection occurs along a continuum from habitual action to deliberate critical inquiry. The deeper end of that continuum requires structured facilitation to reach.
A study by Mamede and Schmidt examining how physicians reflect found that structured reflection significantly improved diagnostic accuracy across a series of clinical case presentations (Mamede & Schmidt, 2004). They identified three distinct modes of clinical reflection: deliberate induction, deliberate deduction, and hypothesis testing. They argued that reflection is not a single behaviour but a family of related cognitive processes. The practical implication is that training programmes need to specify which type of reflection they are developing, not treat it as a generic skill.
The Health and Care Professions Council’s 2019 joint statement, endorsed by multiple UK regulatory bodies, identifies reflective practice as a contributor to self-awareness, the capacity to identify areas for improvement, and sustained professional development over a career (HCPC-UK, 2019). The statement is notable because it moves the argument for reflection from theory into regulatory expectation.
What Reflection Does for the Individual Practitioner
At the individual level, the research identifies several consistent benefits. Practitioners who reflect regularly develop stronger self-awareness: the ability to recognise their own emotional responses, cognitive biases, and decision-making patterns before these create clinical problems. Epstein’s influential JAMA paper on mindful practice argues that attending not only to patient cues but to one’s own internal responses as clinical data is a trainable capacity that improves the quality of both diagnosis and communication (Epstein, 1999).
Reflection also supports metacognition: the capacity to monitor your own thinking and adjust it in real time. In high-stakes environments, this translates to better decision-making under pressure. In direct patient care, it produces more attentive communication and a greater capacity for empathy. For a closer examination of how self-awareness and self-reflection operate as distinct skills in clinical training, see our post on self-awareness vs self-reflection in healthcare.
Gibbs Reflective Cycle
The Gibbs Reflective Cycle, developed by Graham Gibbs in 1988, is one of the most widely used frameworks for structured reflection in healthcare. It guides practitioners through six stages: Description, Feelings, Evaluation, Analysis, Conclusion, and Action Plan, in a sequence designed to prevent superficial reflection. Each stage is made explicit to stop practitioners from noting that something went well or badly without examining why. A survey cited in the British Journal of Midwifery found that 63% of healthcare professionals who used a reflection framework used Gibbs regularly.
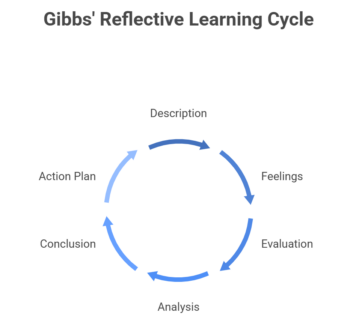
The cycle’s particular strength is its emphasis on feelings as a distinct stage. By separating emotional response from analytical evaluation, Gibbs acknowledges that unprocessed emotion blocks accurate assessment. A trainee who felt embarrassed during a consultation will reflect differently if they first name that emotion rather than trying to suppress it into a neutral account of events. For a full breakdown of each stage and how to apply it, see our guide to the Gibbs Reflective Cycle in healthcare.
Kolb’s Experiential Learning Cycle
David Kolb’s model takes a wider view. Where Gibbs focuses on unpacking a single specific experience in depth, Kolb describes a broader learning cycle in which experience, reflection, conceptualisation, and experimentation feed each other continuously (Kolb, 1984). The four stages are Concrete Experience (the encounter itself), Reflective Observation (reviewing what happened), Abstract Conceptualisation (drawing a transferable conclusion), and Active Experimentation (testing that conclusion in the next encounter).
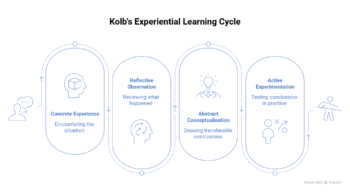
In clinical training, Kolb’s model is particularly useful for understanding why some learners do not transfer simulation performance into clinical practice. A trainee who completes the experience and observation stages but skips conceptualisation, never drawing a general principle from what they observed, will repeat the same patterns in the next scenario. The cycle only closes when active experimentation occurs: the learner commits to a revised approach and tests it. Without that final stage, reflection remains an intellectual exercise without clinical impact.
How Gibbs and Kolb Differ in Practice
The practical difference is one of depth versus breadth. Gibbs is better suited to dissecting a specific, emotionally significant encounter: a difficult consultation, a clinical error, or a moment where communication broke down. It keeps the practitioner with the discomfort of a particular situation until they have extracted something useful from it. Kolb is better suited to understanding how a learner develops across a series of experiences, making it more useful for curriculum design and longitudinal feedback conversations with supervisors.
Immediate vs Delayed Reflection: What the Evidence Recommends
A study by Williams (2012) found that delayed feedback produces stronger learning outcomes than immediate feedback across several important measures. Delayed reflection gives the practitioner time to consolidate the emotional experience before interrogating it analytically, in a sequence that mirrors how long-term memory encodes experience (Williams, 2012). Three mechanisms account for this. First, delayed reflection allows deeper analysis: the practitioner has time to consider the encounter from multiple perspectives rather than reacting to it. Second, it improves retention: internalising the experience before receiving feedback reduces the risk of the feedback displacing the memory. Third, it supports metacognitive development, because the gap between encounter and review creates space for self-assessment before external input arrives.
Immediate debriefs remain valuable, particularly for safety-critical errors that need fast correction. The evidence suggests that the deeper reflective work should follow after a gap. In practice, this means building two-stage feedback into training: a brief immediate debrief to address critical points, then a structured reflective conversation 24 to 48 hours later when both trainee and supervisor can engage with the encounter more analytically.
How to Embed Reflective Practice in Clinical Training
Reflective practice does not develop automatically through clinical exposure. The HCPC-UK joint statement is explicit that reflection benefits from external scaffolding, particularly in early-career practitioners who have not yet developed the habit. Aronson’s practical guide to teaching reflection at all levels of medical education identifies creating psychological safety as the single most important prerequisite: learners will not engage honestly with their own performance in an environment where reflection is used punitively or where vulnerability is penalised (Aronson, 2011). Faculty modelling their own reflective process openly is identified as one of the most effective ways to establish that safety.
Beyond safety, several approaches are well evidenced.
Reflective journals prompt regular written reflection and, when reviewed with a supervisor, produce a record of how a trainee’s thinking develops over time. A qualitative meta-synthesis of health professionals’ and students’ experiences of reflective writing found that writing regularly about clinical encounters supported professional identity formation, deepened empathy, and gave practitioners a structured way to process the emotional demands of difficult clinical work (Artioli et al., 2021). The act of writing forces a level of precision that internal reflection often avoids.
Structured debriefs after simulation sessions give learners a supported environment for applying a framework like Gibbs or Kolb, with a facilitator who can intervene when the reflection stays at the surface. Aronson also recommends introducing staged complexity, beginning with less emotionally charged encounters and progressing to the kind of difficult cases where reflection is hardest but most valuable. Peer observation and discussion, where trainees watch and reflect on each other’s clinical encounters rather than only their own, broadens the reference points available for comparison and reduces the defensiveness that sometimes accompanies self-review.
The Role of Video in Reflective Practice
One of the persistent barriers to effective reflection is recall bias. Practitioners remember interactions differently from how they actually occurred, and the moments most worth reflecting on, particularly those that are emotionally charged, technically demanding, or ambiguous, are often the most distorted in memory. Video review directly addresses this. When a trainee watches a recorded consultation, they have access to what actually happened rather than their reconstruction of it. Patterns that are invisible during the interaction, such as sustained eye contact, shifts in posture, and pacing during a difficult question, become observable and discussable.
Videolab is used for this purpose in clinical education programmes across the Netherlands, Belgium, and the UK. Trainees record consultations via a fixed camera or mobile app, annotate specific moments with time-stamped comments, and share recordings with supervisors or peers for structured reflective feedback. Because recordings are GDPR-compliant and encrypted throughout, the practice can extend to real patient consultations, not only simulations. Reflective learning happens in the context where clinical behaviour actually needs to change.
Frequently Asked Questions
What is reflective practice in healthcare?
Reflective practice in healthcare is the structured process of examining your own clinical actions, decisions, and responses in order to improve future performance. It draws on frameworks like Gibbs’ Reflective Cycle and Kolb’s Experiential Learning Cycle to guide practitioners through a deliberate analysis of their experiences, rather than simply recalling what happened. It is considered a core professional competence by regulatory bodies including the HCPC-UK.
What is the difference between Gibbs and Kolb?
Gibbs focuses on a single specific experience and moves through six stages: Description, Feelings, Evaluation, Analysis, Conclusion, and Action Plan, to extract learning from it in depth. Kolb describes a four-stage cycle of Concrete Experience, Reflective Observation, Abstract Conceptualisation, and Active Experimentation, which applies across a series of experiences and emphasises testing conclusions in practice. Gibbs is better for examining a particular encounter; Kolb is better for understanding how learning develops over time.
When should reflection happen: immediately or later?
Evidence from Williams (2012) supports delayed reflection for deeper learning outcomes. A brief immediate debrief can address critical errors, but the substantive reflective work is more productive after a gap of 24 to 48 hours, when the practitioner can engage analytically rather than reactively. Both stages have a role; immediate debriefs and delayed structured reflection are complementary rather than alternatives.
How do you assess reflective practice in medical education?
The most common assessment methods are reflective portfolios, written case analyses, and structured debriefs with direct observation. Assessment criteria typically evaluate whether the practitioner moves beyond description to analysis, identifying patterns, examining assumptions, and committing to a changed approach. Video-assisted self-review is increasingly used to provide a shared reference point between the trainee and assessor, reducing the subjectivity that can weaken portfolio-based assessment.