
What is shared decision-making in healthcare?
Shared decision-making (SDM) in healthcare is a process in which healthcare providers and patients work together to make decisions about the patient’s care. This means that the patient is not simply told what to do, but is instead involved in the decision-making process. SDM is important because it can help to ensure that patients receive the care that is best for them, given their individual circumstances and preferences.
SDM is founded upon the principle that patients have the right to participate actively in their healthcare decisions. It is also based on the evidence that SDM can lead to better patient outcomes, including increased satisfaction with care, improved adherence to treatment plans, and reduced decisional regret.
In conversation with Haske van Veenendaal on the importance of shared decision making in healthcare, and how it transforms patient-provider communication.
I had the privilege of speaking to a very highly respected expert in the field of shared decision making, Dr. Haske Van Veenendaal. Haske is a researcher and PhD graduate at the Erasmus School of Health & Policy Management, a member of the supervisory board of Mytylschool Gabriel and the owner of an academy which provides shared decision making training, Trant – for the Care of Tomorrow.
His expertise in shared decision-making is extremely interesting, drawing from his extensive experience and profound grasp of the field’s theories, methods, and procedures used in practice.
If you would like to learn more about how shared decision making is taught, its teaching methods, challenges in the field and related topics, listen to the podcast linked below.
A transcript is also available at the bottom of this page.
Additionally, you can find the video podcast on our Youtube linked here.
[lyte id=’_Hxn-Kwjo20′ /]
The information below is based on the insights gained from the interview and other research conducted. All sources cited.
Why is shared decision making in healthcare important?
From research, we can gather that shared decision making in healthcare is very important based on the fact it improves healthcare by fostering a partnership between patients and physicians. It empowers patients to actively engage in decisions about their own health, upholding their autonomy and respecting their rights.
Shared decision making not only elevates patient satisfaction and treatment knowledge but also enhances treatment adherence, potentially leading to improved health outcomes. It is particularly invaluable when multiple treatment options exist and the optimal choice weights on individual factors such as personal preferences or coexisting conditions.
From the perspective of a professional in the field, I also wanted Haske’s opinion on why he thought shared decision making is important, and how it benefits both doctors and patients during a consultation.
He highlighted several main areas where SDM positively impacts consultations. Firstly, for the patient, having a SDM gives them autonomy over the decisions which therefore leads to less regret or upset about decisions being made.
And for doctors, introducing SDM procedures into a consultation allows for more structured conversation, and a more productive interaction with the patient.
Very interestingly enough, Haske also mentioned it also helps clinicians feel less responsible for the outcome of treatments. By sharing responsibility, the doctor can be confident that the patient has carefully considered the treatment options and is prepared for different possible outcomes.
Are there any specific frameworks or models that are used in a shared decision making consultation?
Haske meticulously outlined the general structure employed before and during a shared decision-making consultation.
Physicians first strategise for the consultation, outlining potential discussions and decisions tailored to the patient’s individual case.
From there, the doctor typically follows five steps.
- Introduction to the decision that is to be made, clearly understanding your role as the clinician, and the role of the patient during the process of joint decision making.
- Access and discuss positives and negatives of the options presented to the patient and make sure the patient fully understands what is being discussed.
- Determining what is important to the patient, what their preferences, values and priorities are throughout the procedure.
- Finding and agreeing on a decision that is supported by both the patient and clinician, taking in both the clinicians expertise in the field, and the patient’s wishes.
- The final step would be to evaluate the choices that have been made that are in line with the result both parties are wanting to achieve.
Note, Haske mentioned that this model can change depending on important factors of the patient. In practice, “it’s all about the specific context in which the clinician works”.
Doctors must deal with each case slightly differently, a cancer patient’s care is very distinct from a child’s care, such as chronic patients are from acute patients.
Doctors must have the training and ability to modify communication and behaviour of the shared decision making techniques in different contexts and healthcare settings. Training must properly prepare doctors with these skills.

Strategies to help implement shared decision making in an organisation
Haske finished his PhD this year on the “Implementation of shared decision making in daily healthcare in clinical oncology care“.
The study involved interviewing experts at a high level who already had experience in effectively implementing SDM in their practices to gather insights and recommendations for wider adoption. These professionals collaborated with 11 teams of hospitals to develop and implement multilevel SDM strategies over approximately a year.
These multilevel strategies involved the training of clinicians, looking at the organisational structure, and looking at the context in which they need to function such as the guidelines, resource allocation changes and financial influence.
The structure of implementation would need to change for each organisation type depending on the layout of the business plan.
From the research done by Haske and his colleagues, the results found that when applied properly, the multilevel implementation strategy proved to be a very effective approach to shared decision making.
6 strategies to help implement shared decision making based on National Learning Consortium, Shared Decision Making Fact Sheet. (2013)
- Invite the patient to participate: inviting patients to participate through questions allows them to voice their opinions at an early stage, helping build trust.
- Present options: patients need to be aware of the whole process that has occurred before presenting diagnosis and treatment options. Explain this process to them.
- Provide information on benefits and risks: Share impartial information from existing scientific evidence. Follow up with patients to ensure their understanding of the provided information.
- Assist patients in evaluating options: Help patients assess their options by considering their goals and concerns. Inquire about what matters most to patients and what worries them to gain insights into their preferences.
- Facilitate deliberation and decision making: Let the patients know they have time to think things over. Ask patients if there is any additional information or action they require before they can confidently make a decision.
- Support patients in implementing their decision: outline the subsequent actions they need to take. Confirm their comprehension and address any potential obstacles they may encounter while executing the decision.
How do oncology patients feel about shared decision making?
During Haske’s PhD, the researchers surveyed cancer patients to understand their experiences with SDM and their preferences in decision-making processes. They found a very interesting and surprising result. After questioning, they found that up to more than 80% of the oncology patients also wanted to discuss the option of no treatment within the diagnosis options.
Do shared decision making practices increase consultation time?
In a separate part of Haske’s PhD research, another study examined a significant barrier to shared decision making.
Shared decision-making consultations are generally perceived to require more time than consultations without SDM structure or methods.
To address this common concern, they conducted a comprehensive review of studies and found that contrary to expectations, SDM does not necessarily prolong consultations. In fact, many studies showed no significant increase in consultation duration. Twenty-eight of the 35 studies we selected did not show an increase in consultation time, suggesting that SDM can be incorporated into routine clinical practice without compromising efficiency.
Haske commented that despite evidence that SDM does not necessarily prolong consultations, there’s a lingering question about whether the initial implementation of SDM practices may temporarily increase consultation duration.
However, it’s expected that this increase would diminish as practitioners become accustomed to the new approach.
Why did Erasmus MC choose Videolab to help with shared decision making training?
Erasmus MC university was our first customer in the Netherlands, adopting Videolab in 2017, first in their GP department, then to facilitate the training of both clinical and communication skills a few years later.
So, why did they choose Videolab?
As Haske explained during the interview, The Netherlands regularly train their medical students using real patient consultations and situations.
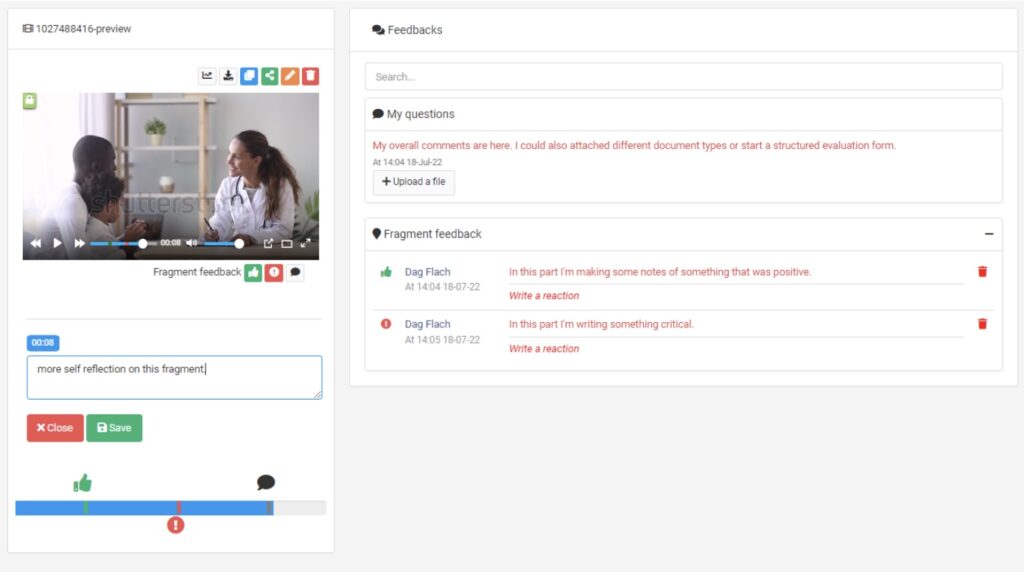
Given the opportunity to record a series of consultations for feedback purposes and coaching provides huge value in training. Not only limiting this tool to students training, but also very much applies to helping training clinicians in an ever changing medical environment. They needed a tool which allowed them to safely record patients and to review and assess these recordings. This is where Videolab came in, providing Erasmus MC with the solution to record consultations while keeping privacy by design in front of mind, securing patient data. Also allowing students to watch back this recording in their own time, and reflect on their performance, then share with assessors for further feedback and evaluation.
Communication techniques are constantly changing, Haske recommends that clinicians should also go through consistent training to aid the practice and application of new methodologies. He believes that such a system as Videolab helps the training of communication competencies and benefits the overall healthcare environment.
Where else could Videolab be used in the future?
Videolab is already used in many places, and it has become the go-to tool for doctor patient communication training and consultation training.
As mentioned above, healthcare is constantly undergoing transformative innovations pushed by technological advancements and the growing emphasis on patient-centred care.
Haske explained two very important factors in healthcare.
The first being equality, we all have our own qualities and expertise, we also all have the right to make autonomous decisions. Patients need to feel equal in and during a consultation or healthcare procedure.
The second being, we are all unique. We must recognize our inherent differences. Clinicians must acknowledge that each patient and situation is very different.
Videolab fosters the training of a personalised approach to healthcare, ensuring that each patient receives the care they need, tailored to their specific circumstances. It’s not about adhering to rigid protocols or predetermined approaches; it’s about understanding the nuances of each individual and tailoring care accordingly.
Interested in how Videolab supports training for shared decision making in healthcare?
[sp_easyaccordion id=”3696″]