

A summative decision must withstand scrutiny. The feedback attached to it must also help the learner improve. Clinical education often asks one short narrative to do both jobs.
That is difficult when an assessment affects progression, entrustment, or remediation. A vague comment may be kind but educationally empty. A list of faults may justify a low score but give the learner no realistic priority. Strong summative feedback connects the standard, the observed performance, the decision, and the learner’s next opportunity to improve.
What is summative feedback?
Summative feedback is information provided with or after a formal judgment of performance at the end of a defined assessment period. It explains how the learner performed against the relevant standard, why the assessor reached the decision, and what the learner should carry into the next performance.
The assessment and the feedback are related but distinct. A summative assessment produces a grade, score, pass, entrustment level, or progression decision. Summative feedback explains the evidence behind that outcome. A number records the result. A useful narrative makes the result intelligible.
Wood and Jones found that this distinction often becomes blurred. Their analysis of feedback on 105 assignments across 16 degree programs showed that comments commonly identified deficiencies or justified grading decisions rather than engaging with the learner’s ideas. They argued for clearer separation between feedback that justifies a grade, advises the learner, and challenges the learner’s thinking. Their study of summative feedback exposes the central design problem: one narrative may serve institutional and educational purposes, but those purposes must be explicit.
Summative feedback has two jobs in clinical education
Good summative feedback creates both a defensible record of the decision and a developmental handover to the learner’s next assessment or clinical setting.
Job 1: Make the decision defensible
The narrative should show how the decision follows from agreed criteria and observed performance. This does not mean rewriting the rubric. It means identifying the evidence that mattered and explaining how it affected the judgment.
Defensibility is particularly important when the learner fails, receives a borderline result, or is judged not ready for greater independence. In those cases, the feedback should distinguish a safety-critical omission from a general impression. It should also avoid personality labels such as unconfident, disorganized, or not professional enough unless the assessor can name the behavior that supports the conclusion.
Job 2: Hand over a priority for future performance
The completed task cannot be changed, but the learner’s next performance can. The feedback should therefore identify what to retain, what to change first, and where the learner can apply that change.
Svensäter and Rohlin demonstrated this dual purpose in a dental program. Their model used linked formative and summative assessments to judge students’ level of understanding and development over time. Students received individual feedback after the summative assessment, and the participating students valued seeing how their understanding had developed. The dental education study shows that judgment and development do not need to compete when the assessments are designed as part of a sequence.
How to write summative feedback in four parts
A reliable summative comment can be built from four parts: criterion, observed evidence, judgment, and next performance.
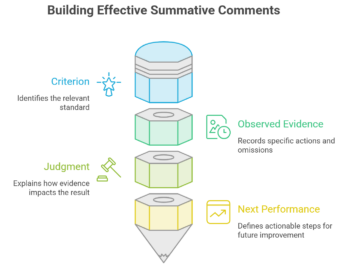
1. Name the criterion that matters
Start with the relevant competency, learning outcome, or assessment criterion. Select the criterion that drove the decision rather than listing every domain on the form.
For example: This judgment relates to information gathering and clinical safety. That opening tells the learner and any reviewer which standard the comment addresses.
2. Describe the observed evidence
Record what the learner did, said, or omitted. Avoid converting an observation into a trait.
You did not ask about anticoagulant use before recommending treatment is observable. Your history taking was careless is an inference. The first can support a decision and a learning plan. The second is difficult to verify and harder to act upon.
Natesan and colleagues recommend that clinical feedback should be clear, specific, timely, actionable, and based on observed behavior. They also recommend including both reinforcing and corrective information. Their evidence-based medical education review supports grounding the narrative in performance rather than personal judgment.
3. Explain the judgment
State how the evidence affected the result. If one omission caused a failure despite otherwise competent performance, say so. If repeated observations produced the judgment, describe the pattern.
For example: Although the consultation was otherwise organized, the missed medication check created a safety risk and therefore did not meet the station’s mandatory safety criterion.
This sentence does not soften the result. It makes the logic transparent and prevents one failed criterion from being mistaken for a judgment about the learner’s entire capability.
4. Define the next performance
End with one priority that can be observed in a later task. Revise medication safety is a topic, not an action. Before proposing treatment in your next three observed consultations, complete and verbalize a medication and allergy check gives the learner a behavior, context, and opportunity for review.
Perera, Nguyen, and Watty describe feedback as feedforward when comments carry clear implications for future tasks. Their study found an association between feedback embedded in recurring summative activities and later performance, although attendance, participation, and feedback were intertwined. The recurring assessment study supports connecting comments to a later opportunity while cautioning against attributing improvement to feedback alone.
Summative feedback examples from clinical assessment
The strongest examples show the decision and the developmental priority without confusing one for the other.
A failed OSCE with otherwise strong performance
Weak: Generally good station, but you missed an important safety point. Review prescribing.
Stronger: You gathered the presenting history in a logical sequence and explained the proposed treatment clearly. However, you did not ask about allergies before recommending medication. This omission did not meet the mandatory prescribing-safety criterion and resulted in a station fail. Before proposing medication in your next observed station, pause and verbalize checks for allergies, current medicines, and contraindications.
The stronger version preserves evidence of competence, explains why the omission determined the result, and defines what the assessor should look for next time.
An end-of-placement judgment based on mixed observations
Weak: Performance was inconsistent. Needs more confidence and independence.
Stronger: Across four documented case presentations, you gathered relevant information and identified appropriate initial investigations. In three presentations, you waited for supervisor prompts before stating and prioritizing a differential diagnosis. You have met the standard for information gathering but not yet for independent clinical synthesis. On your next placement, present your three leading diagnoses and the evidence for each before asking for supervisor input.
This version identifies the evidence base, separates two competencies, and avoids using confidence as a substitute for observable performance.
An EPA decision with a limit on independence
Weak: Can perform with indirect supervision but should continue to gain experience.
Stronger: You completed routine discharge planning accurately in the five reviewed cases and sought help appropriately when social risk complicated the plan. The evidence supports indirect supervision for routine cases. Cases involving safeguarding concerns still require direct review. For the next entrustment decision, document two safeguarding cases in which you identify the concern, initiate the pathway, and explain when senior input is required.
The feedback defines the boundary of the entrustment decision. It also specifies what evidence could support a later change in supervision.
A recorded consultation
Weak: Good empathy, but you missed some emotional cues.
Stronger: You acknowledged the patient’s concern when they first described the pain. At 06:40, when the patient said they were worried about losing their job, you moved directly to the management plan. This limited exploration of the concern and did not fully meet the response-to-cues criterion. In your next recorded consultation, respond to an emotional cue with acknowledgment and one exploratory question before returning to clinical planning.
A recording can anchor the comment to a reviewable moment. Natesan and colleagues identify video-assisted feedback as a useful extension of direct observation while noting that recording may influence behavior and cause anxiety. Their review supports treating video as evidence with limitations, not as an unquestionable record of usual performance.
How should difficult summative decisions be documented?
Difficult decisions require greater precision, not more severe language.
When the result is borderline
State which evidence supports meeting the standard and which evidence creates doubt. Then explain the rule or threshold used to reach the final decision. Do not disguise uncertainty with a vague phrase such as just about passed.
When assessors disagree
Describe the pattern and context of the observations before presenting the resolved judgment. A disagreement may reflect different cases, levels of support, or opportunities to observe the competency. Natesan and colleagues recommend standardized, structured, multisource, and longitudinal feedback processes in medical education. Their recommendations support collecting evidence across people and settings rather than relying on an isolated global impression.
When the learner has failed
Separate the assessment consequence from the development plan. First, state what did not meet the standard and why. Then prioritize the behavior that must change before reassessment. A long catalogue of every weakness can make the core reason for failure harder to identify.
When the same task will not recur
Connect the feedback to the next analogous performance. A final pediatric placement may not repeat, but the learner will still gather histories, communicate risk, prioritize differentials, and seek supervision elsewhere. The next action should transfer at the level of the competency, not depend on repeating an identical task.
How can programs improve the quality of summative comments?
Programs improve summative feedback by treating narrative quality as part of assessment quality, not as an individual assessor’s writing preference.
- Use shared criteria: Assessors should work from the same performance standards and understand which criteria can determine failure or progression.
- Calibrate with examples: Faculty should compare sample narratives and discuss whether the evidence supports the stated judgment.
- Structure the form: Separate fields for criterion, evidence, judgment, and next performance reduce the temptation to write an unsupported global comment.
- Review a sample: Moderation should examine narrative comments as well as scores, particularly in failed and borderline cases.
- Allow learner response: Learners should have a route to clarify the feedback, record their interpretation, or agree on the next priority.
- Carry one priority forward: Where policy permits, the next supervisor should be able to see the development target without receiving an indiscriminate archive of past judgments.
Wood and Jones found marked variation in the quantity, emphasis, and purpose of comments within one curriculum area. They concluded that confused feedback practices reflected tension between institutional expectations and educational principles. Their findings make a strong case for program-level decisions about what summative feedback is supposed to accomplish.
For help selecting a conversational structure after the written judgment is complete, see our guide to implementing feedback models. For the broader distinction between assessment-stage purposes, see formative vs summative feedback.
A quality check for summative feedback
Before releasing a summative narrative, check whether it answers these eight questions:
- Which criterion or competency drove the decision?
- What did the learner actually do, say, or omit?
- Does the evidence justify the stated judgment?
- Have I separated observation from inference?
- Is one behavior worth retaining made explicit?
- Is the priority for improvement clear?
- Can that priority be observed in a future performance?
- Could another assessor understand and defend this decision?
Summative feedback should not attempt to teach everything after the assessment has ended. Its job is narrower and more demanding: make the decision transparent, preserve the evidence that matters, and hand the learner a credible next step.
Frequently Asked Questions
What is an example of summative feedback?
A useful example explains a final OSCE result with observed evidence: You did not check allergies before recommending medication, so the performance did not meet the mandatory safety criterion. In your next observed station, verbalize allergy, medication, and contraindication checks before proposing treatment.
Is a grade considered summative feedback?
A grade is a summative judgment, but it provides little feedback by itself. Summative feedback explains which evidence produced the grade and what the learner should retain or change.
Can summative feedback support future learning?
Yes. Feedback on a completed assessment can guide future learning when it identifies a transferable behavior and a later opportunity to demonstrate it.
Videolab helps clinical education teams link summative judgments to reviewable evidence from recorded OSCEs, simulations, and consultations. Assessors can cite specific moments, compare them against shared criteria, and preserve an auditable connection between what happened, why it affected the decision, and what the learner should demonstrate next.