

Choosing a feedback model is not an administrative decision. The framework a clinical educator uses shapes what gets said, who speaks first, how emotions are handled, and whether the learner leaves with something they can act on. Seven models are in common use across medical education, each designed for a different context, a different learner profile, and a different outcome. This post explains how each works, where each fits, and what the research supports.
Why Feedback Model Selection Matters
Feedback is one of the most studied interventions in education. Hattie and Timperley’s synthesis of over 800 meta-analyses found feedback has an effect size of 0.73, placing it among the highest-impact educational interventions identified (Hattie & Timperley, 2007). That effect size is not automatic, however. Van de Ridder and colleagues identified that feedback in clinical education only reliably improves performance when it is specific, based on observable behaviour, delivered promptly, and given in an environment where the learner can respond (van de Ridder et al., 2008). The model used determines whether those conditions are met.
Branch and Paranjape argue that feedback and reflection are mutually reinforcing. Structured reflection deepens how learners integrate and act on the feedback they receive, while good feedback provides the specific material reflection needs to work with (Branch & Paranjape, 2002). The implication for model selection is that the best frameworks do not simply deliver a verdict on performance. They create the conditions for the learner to reflect on it.
Morris and colleagues’ systematic review of formative assessment in higher education confirms that three conditions consistently determine whether feedback leads to learning: feedback quality, student agency in interpreting and responding to it, and the presence of genuine dialogue rather than one-way transmission (Morris et al., 2021). Each model below performs differently across those three dimensions.
The Feedback Sandwich
The Feedback Sandwich opens with a positive observation, introduces the area for improvement, and closes with further positive reinforcement. It is the most widely used feedback format in clinical education, partly because it is easy to learn and quick to apply in time-pressured settings. The intention is to protect the learner’s confidence while still delivering the critical point.
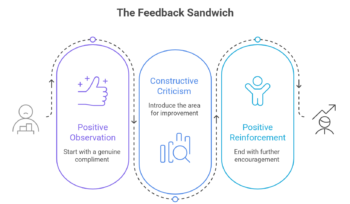
The evidence on its effectiveness is mixed. The structure can dilute the impact of the critical feedback: learners often retain the positive bookends and discount the central point. It can also feel formulaic to more experienced practitioners who recognise the pattern immediately. Despite these limitations, it has a genuine role when the feedback relationship is new and learner confidence is fragile.
Best for: Introduction to Clinical Skills sessions, early simulation encounters, and any setting where the observer and learner are meeting for the first time.
Pendleton’s Rules
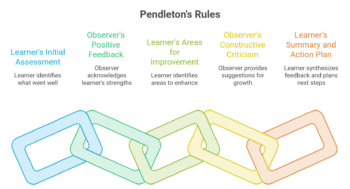
Pendleton’s Rules invert the typical feedback dynamic by requiring the learner to speak first (Pendleton et al., 1984). The sequence is as follows: the learner states what went well; the observer states what went well; the learner states what could be improved; the observer states what could be improved; the learner summarises and forms an action plan. By asking the learner to commit to a position before receiving external input, the model prioritises self-reflection and ownership of learning outcomes.
The rationale has empirical support. Eva and Regehr’s review of self-assessment in the health professions found that internal self-evaluation is often inaccurate on its own. Externally assisted self-assessment, where learners engage with their own performance before receiving observer input, is significantly more effective than either unaided self-evaluation or observer-led feedback alone (Eva & Regehr, 2005). Pendleton’s structure operationalises exactly this: the learner generates their analysis first, then calibrates it against the observer’s.
The main limitation is that a learner who starts with an inaccurate self-assessment can pull the session in the wrong direction if the observer is not confident about redirecting. This makes Pendleton’s Rules more suitable for postgraduate settings than early undergraduate training. For a detailed breakdown of the model, see our guide to Pendleton’s Rules.
Best for: Postgraduate training, self-directed learning programmes, Internal Medicine, and Emergency Medicine rotations.
The ECO Model
The ECO Model addresses emotion before content. Its three stages of Emotion, Content, and Outcomes are ordered deliberately. The observer first invites the learner to express their emotional response to the encounter, validates it, and only then moves to discussing clinical content and establishing a plan.
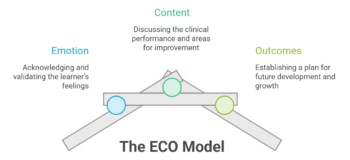
The rationale is grounded in cognitive psychology. Emotional arousal inhibits analytical processing: a learner who is anxious, defensive, or visibly upset about a performance cannot receive specific developmental feedback effectively until that emotional state has been acknowledged. Attempting to move straight to content under those conditions tends to produce passive compliance rather than genuine engagement. The ECO Model creates the conditions for feedback to land.
Best for: Feedback following high-stress clinical encounters, end-of-life conversations, critical incidents, or any session where the learner showed visible distress. Particularly valuable in palliative care, oncology, and emergency training.
Multi-Source Feedback
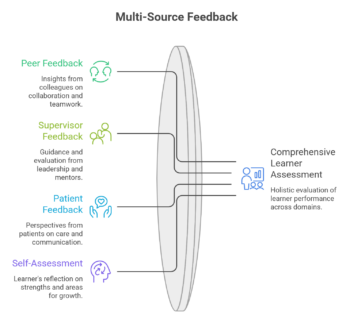
Multi-Source Feedback (MSF), sometimes called 360-degree feedback, collects input from multiple observers: peers, supervisors, patients, and the learner’s own self-assessment, then synthesises them into a structured report. Lockyer’s review of MSF as an assessment tool found it to be a valid and reliable method for evaluating physician competencies across professional, interpersonal, and clinical domains, with particular strength in surfacing patterns of professional behaviour that a single supervisor cannot detect (Lockyer, 2003). The value is in the breadth of perspective: a single observer’s assessment reflects that observer’s priorities and blind spots. MSF captures a learner’s performance across contexts and roles, making it harder to dismiss as individual opinion.
The logistical demands are significant. Collecting, processing, and debriefing multi-source data requires infrastructure that many clinical training programmes cannot easily provide. When that infrastructure exists, however, MSF is the most comprehensive picture of a learner’s clinical behaviour available.
Best for: Clinical rotations and internships where a trainee interacts with multiple teams and disciplines. Particularly useful for identifying patterns in professional behaviour that only become visible at scale.
The R2C2 Model
The R2C2 Model, developed by Sargeant and colleagues, addresses one of the consistent failure modes of MSF: data without dialogue. Four stages guide the conversation: Relationship, Reaction, Content, and Coaching. The facilitator first establishes a safe relationship with the learner, then invites and validates the learner’s emotional reaction to the feedback data, then moves to examining the content of the report in detail, and finally shifts into coaching mode to help the learner identify specific changes (Sargeant et al., 2015).
The model was tested in physician practices receiving multisource feedback and found that structured facilitation using R2C2 significantly improved how physicians engaged with and acted on their results compared to receiving the report without facilitation. The key mechanism is the explicit attention to emotional reaction before analytical content, following the same logic as the ECO Model extended into a longer facilitated conversation. R2C2 is not a standalone feedback format for a single encounter; it is a framework for the debrief conversation that follows a formal assessment process like MSF or programmatic feedback.
Best for: Debriefing MSF results, end-of-rotation reviews, and any structured feedback conversation where the learner is receiving data from multiple sources and needs support to interpret and act on it.
The Feedback Literacy Model
Developed by Carless and Boud, the Feedback Literacy Model shifts attention from what the observer delivers to what the learner can do with it (Carless & Boud, 2018). It identifies four capacities: appreciating the value of feedback, making judgements about one’s own work, managing emotional responses to feedback, and taking action on what has been received. The model is less a procedure than a curriculum. Its goal is to produce learners who can seek out, evaluate, and act on feedback throughout their careers, rather than remaining passive recipients who only engage when an observer initiates the process.
Eva and Regehr’s work on self-assessment provides the empirical basis for this approach: because internal self-evaluation is unreliable without external calibration, the most durable form of feedback competence is not accuracy in self-assessment per se, but the capacity to actively seek, interpret, and use external input over time. Feedback literacy describes exactly that capacity.
The limitation is that it requires sustained investment in the feedback relationship and does not produce the quick, observable improvements that other models can generate in a single session. It is most effective when embedded across a whole rotation rather than used in isolated encounters.
Best for: Clinical rotations and internships where long-term professional development and self-directed learning are explicit training goals. Pairs well with reflective portfolios and structured peer review.
The MISCA Model
The MISCA Model frames feedback as an interaction between five elements: Message, Implementation, Students, Context, and Agents. Where other models focus on the exchange between one observer and one learner, MISCA acknowledges that feedback always operates within a system. The same feedback, delivered by different people, about different skills, in different institutional contexts, will have different effects on different learners. The model does not prescribe a procedure. It provides a diagnostic framework for understanding why feedback is or is not working.
MISCA is most useful for programme-level decisions: designing feedback policies, training feedback providers, and evaluating why feedback is failing consistently across a cohort.
Best for: Continuing medical education, programme design, and institutional quality improvement. Less suited to individual encounter feedback; more suited to the educators who are designing feedback systems.
Practical Comparison
| Model | Who speaks first | Emotion handled | Best applied in |
|---|---|---|---|
| Feedback Sandwich | Observer | Implicitly (through framing) | Early training, new relationships |
| Pendleton’s Rules | Learner | Not explicitly | Postgraduate, self-directed programmes |
| ECO Model | Learner (emotional) | Explicitly, first | High-stress encounters, palliative care |
| MSF | Multiple observers | In debrief session | Rotations, multi-team environments |
| R2C2 | Facilitator (relationship) | Explicitly, second stage | MSF debrief, end-of-rotation reviews |
| Feedback Literacy | Learner (self-assessment) | As a named competency | Internships, longitudinal programmes |
| MISCA | Programme level | At system level | Curriculum design, faculty development |
Choosing the Right Model
A few practical principles clarify the choice. Use the Feedback Sandwich or Pendleton’s Rules for individual encounters in formative training: Feedback Sandwich when the relationship is new, Pendleton’s when self-reflection is the primary goal. Use the ECO Model when emotional content is likely to dominate the conversation. Use MSF when you need a complete picture of a learner’s professional behaviour across contexts; pair it with R2C2 for the debrief to ensure the data translates into action. Use the Feedback Literacy Model when the goal is to develop learners who can function independently. Use MISCA when feedback is failing systemically and you need to diagnose why at the programme level.
For the broader distinction between feedback that supports ongoing learning and feedback that evaluates final performance, see our post on formative vs summative feedback.
Embedding Feedback Models in Clinical Training
Awareness of a model is not the same as competence in applying it. An observer who has read about Pendleton’s Rules but never practised them will default under pressure to unstructured commentary or the Feedback Sandwich, the path of least resistance. Faculty development that includes applying each model in observed role-play, receiving feedback on how it was delivered, and debriefing the process afterward is the most reliable route to consistent practice.
Natesan and colleagues’ evidence-based guide to feedback in medical education identifies the feedback relationship as the prerequisite for all other conditions. Without psychological safety, neither specificity nor timing nor model choice will produce reliable learning (Natesan et al., 2024). This is a programme-design concern, not just a faculty development one: training environments that use feedback punitively or inconsistently undermine model effectiveness regardless of which framework is used.
Kogan and colleagues’ review of direct observation tools argues that observation remains the gold standard for clinical skills assessment, and that feedback quality is directly constrained by the quality of the observation preceding it (Kogan et al., 2009). The mini-CEX and DOPS in particular are designed to make observation structured and repeatable. When these tools are used consistently, the feedback conversation has a shared reference point, which makes models like Pendleton’s Rules and R2C2 significantly easier to apply well.
Videolab supports this by making clinical encounters available for review in ways that extend beyond what direct observation alone permits. When a supervisor can watch a recorded OSCE debrief or simulation feedback session, they can evaluate not just what the learner did but how the feedback itself was structured: whether it was specific, whether it created space for the learner to respond, and whether the model was applied as intended. This turns feedback training into the same evidence-based, reviewable process that it asks clinical skills training to be.
Frequently Asked Questions
What is the most effective feedback model in medical education?
There is no single most effective model. Effectiveness depends on context, learner stage, and feedback goal. Hattie and Timperley’s research identifies feedback that is specific, timely, and focused on the task rather than the person as consistently high-impact. Pendleton’s Rules and the Feedback Literacy Model tend to produce stronger self-directed learning outcomes; the ECO Model is more effective in emotionally charged situations; MSF provides the most complete picture across a rotation. Matching the model to the context matters more than selecting any single default.
What are Pendleton’s Rules?
Pendleton’s Rules are a feedback framework in which the learner speaks before the observer. The sequence asks the learner to identify what went well, then the observer adds to that; the learner then identifies what could be improved, and the observer builds on that. The learner closes with an action plan. The model was developed by Pendleton and colleagues in 1984 specifically for the medical consultation context and is widely used in postgraduate clinical training. For a full explanation, see our guide to Pendleton’s Rules.
What is multi-source feedback in healthcare?
Multi-source feedback (MSF), also called 360-degree feedback, collects structured assessments from multiple people who have observed a trainee’s performance, including peers, supervisors, and sometimes patients. The responses are compiled into a report that reflects the trainee’s professional behaviour across roles and contexts. It is most commonly used during clinical rotations and internships, where a single supervisor cannot observe all aspects of a trainee’s practice. The R2C2 model is specifically designed for facilitating the debrief conversation that follows an MSF report.
How does the ECO Model differ from the Feedback Sandwich?
Both models acknowledge that emotional state affects how feedback is received. The difference is in how they respond to it. The Feedback Sandwich uses positive framing to soften the emotional impact of critical feedback. It works around emotion. The ECO Model names and validates the learner’s emotional response explicitly before moving to content. It works through emotion. ECO is more appropriate when the emotional content is significant enough that ignoring it would prevent the feedback from landing.