

Crisis intervention is one of the most demanding communication tasks in clinical practice. A patient in acute distress, a family member in psychological shock, or a person presenting to the emergency department in the aftermath of a traumatic event — these situations require more than empathy. They require structure.
Roberts’ Seven-Stage Crisis Intervention Model, developed by Albert R. Roberts and refined across several editions of his foundational text Crisis Intervention Handbook (1991, 2005), provides that structure. It is widely taught in nursing, social work, psychiatry, emergency medicine, and crisis counselling training globally — and for good reason. It moves the practitioner through a clear sequence, from initial assessment to follow-up, in a way that neither reduces the complexity of a crisis nor leaves the clinician without a map.
This guide explains each of the seven stages, how to apply them in healthcare contexts, and where the model fits alongside other clinical communication frameworks.
What Is Roberts’ Crisis Intervention Model?
Roberts’ model is a sequenced framework for de-escalating acute psychological crises and restoring the person’s functional stability. Unlike models designed for routine communication (such as SPIKES for breaking bad news, or Calgary-Cambridge for consultation structure), Roberts’ model is specifically built for situations where a person’s coping capacity has been overwhelmed — where normal problem-solving has broken down and immediate clinical support is required.
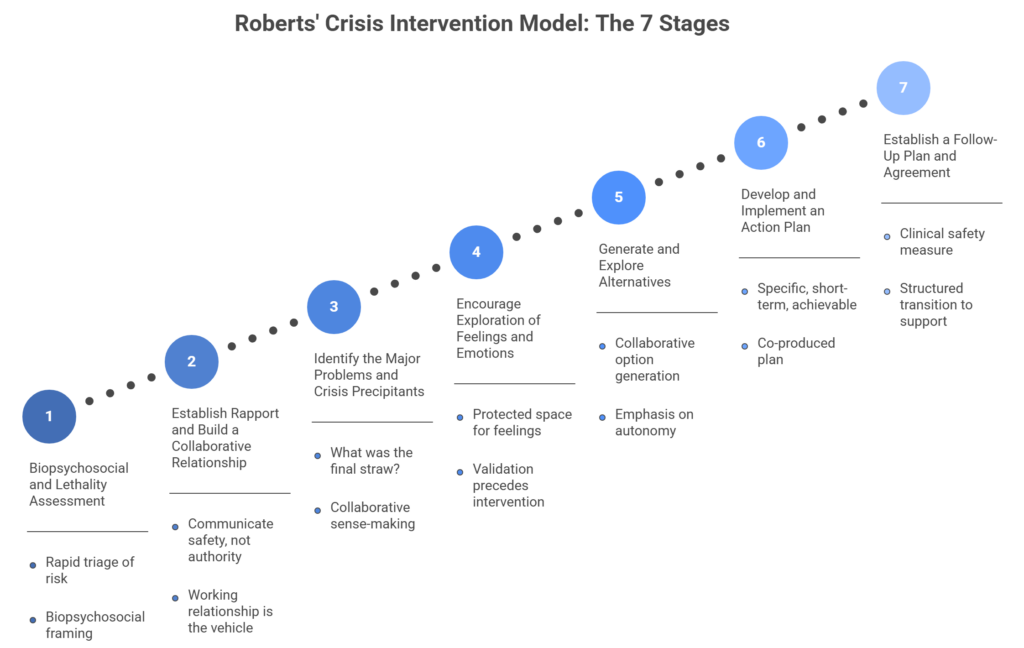
The seven stages move from structured assessment through to the restoration of pre-crisis functioning, with deliberate attention to both immediate safety and longer-term planning. The stages are:
- Plan and conduct a thorough biopsychosocial and lethality assessment
- Establish rapport and rapidly build a collaborative relationship
- Identify the major problems and the crisis precipitants
- Encourage exploration of feelings and emotions
- Generate and explore alternatives
- Develop and implement an action plan
- Establish a follow-up plan and agreement
Each stage is described below.
The Seven Stages in Detail
Stage 1: Biopsychosocial and Lethality Assessment
Before any intervention begins, the clinician assesses the person’s immediate safety and overall presentation. This is not a full psychiatric assessment — it is a rapid triage of risk. Is the person at risk of harming themselves or others? Are there immediate physical safety concerns? What is their mental state: are they oriented, coherent, able to engage?
The biopsychosocial framing is important here. Roberts explicitly includes biological factors (substance use, medical history, pain), psychological factors (mood, cognition, prior mental health history), and social factors (housing, support networks, recent losses) as equally relevant to understanding what has precipitated the crisis. This comprehensive lens prevents the common clinical error of treating a crisis as a purely psychological event.
Stage 2: Establish Rapport and Build a Collaborative Relationship
Build rapport quickly and deliberately. In crisis situations, people often feel dysregulated and may distrust clinicians, especially in emergency settings where previous healthcare encounters have been negative. The clinician should communicate safety, not authority.
Clinicians do this by listening actively, matching the person’s pace instead of imposing clinical efficiency, using their name, and showing that they take the person’s experience seriously. Roberts emphasizes that the working relationship does not sit beside the intervention. It drives every stage that follows.
Stage 3: Identify the Major Problems and Crisis Precipitants
Once safety is established and rapport is developing, the clinician works to understand what has actually happened. What was the final straw? What brought this person to this point now? The distinction between background stressors (chronic difficulties) and the immediate precipitant (the specific event that overwhelmed coping) is clinically significant: the intervention needs to address the precipitant, not just the pattern.
This stage involves careful questioning and listening. It is not an interrogation — it is collaborative sense-making. The goal is to help the person identify and articulate what has happened, which itself often begins to restore a sense of cognitive order.
Stage 4: Encourage Exploration of Feelings and Emotions
Clinical settings often suppress emotional expression in the name of efficiency. Roberts’ model explicitly reverses this. Stage 4 creates protected space for the person to express what they are feeling without those feelings being immediately problem-solved or normalised away.
This stage matters for clinical reasons, not just humanitarian ones. Unexpressed or suppressed emotion in a crisis state does not dissipate — it delays engagement with the later stages of the model. The clinician who moves too quickly to problem-solving before emotions have been acknowledged will find the person disengaged or escalating rather than stabilising. Validation precedes intervention.
Stage 5: Generate and Explore Alternatives
Once the precipitant is understood and emotions have been acknowledged, the clinician shifts to a forward-looking mode: what options exist? This stage is collaborative. The clinician does not present a pre-prepared solution — they work with the person to identify realistic alternatives to the situation, including coping strategies, support resources, and immediate practical steps.
The emphasis on generating rather than prescribing alternatives is deliberate. Autonomy is a component of psychological safety, and a person who has actively participated in identifying their options is more likely to follow through on them than one who has been told what to do.
Stage 6: Develop and Implement an Action Plan
Stage 5 generates options; Stage 6 selects and commits to one. The action plan is specific, short-term, and achievable — it focuses on what will happen in the next hours or days, not on long-term therapeutic goals. It typically includes immediate safety measures, contact points, and concrete next steps.
Importantly, the plan is co-produced. The clinician’s role is to structure and support its development, not to dictate it. This preserves the collaborative relationship established in Stage 2 and is consistent with evidence on treatment adherence: people follow through on plans they have helped to create.
Stage 7: Establish a Follow-Up Plan and Agreement
The final stage extends the intervention beyond the immediate encounter. When will there be a check-in? Who will the person contact if the crisis re-escalates? What services or supports are now in place? Follow-up is not administrative — it is a clinical safety measure. It communicates ongoing concern and provides a structured bridge between crisis intervention and ongoing care.
Roberts’ insistence on follow-up as a formal stage of the model reflects the research on crisis resolution: a single de-escalation encounter rarely produces lasting stability without a structured transition to continuing support.
A Clinical Example
A 34-year-old man is brought to the emergency department by a friend after sending a distressing message and not responding to calls. He is agitated, speaks in fragmented sentences, and makes minimal eye contact.
The nurse assessing him begins:
- Stage 1: there are no weapons, no immediate medical emergency, but he has expressed thoughts of self-harm. She documents the lethality level as moderate and proceeds.
- Stage 2: she introduces herself by first name, sits at the same level, and makes no demands for the first two minutes. She acknowledges that this must have been a frightening night.
- Stage 3: through open questions, she learns that he lost his job three days ago — the precipitant — compounding a period of financial strain and social isolation that has been building for months.
- Stage 4: she does not move to problem-solving when he begins to cry. She allows the silence. He says no one has let him do this before.
- Stage 5 and 6: together, they identify that he has one friend he trusts, that he is willing to call the crisis line if thoughts intensify, and that his GP appointment — previously cancelled — will be rescheduled tomorrow.
- Stage 7: the nurse arranges a welfare call for the following morning and provides written contact details for the on-call mental health team.
This is what the model looks like when applied as intended: not as a checklist, but as a clinical conversation with a clear developmental logic.
Strengths and Limitations
Roberts’ model is comprehensive in a way that shorter frameworks are not. Its inclusion of lethality assessment and biopsychosocial context in Stage 1 addresses the clinical risk management dimension that purely communication-based models omit. The explicit follow-up stage addresses one of the most common failures in crisis care: the gap between acute intervention and ongoing support.
oberts’ model has one major limitation: time. Clinicians need longer than brief crisis contacts often allow to work through all seven stages properly, especially in busy emergency departments, telephone triage, or walk-in settings. For very brief interactions, clinicians may find the Collaborative Assessment and Management of Suicidality (CAMS) framework or the SAFER-R model more practical. Roberts’ model works best when the clinician has at least 30–60 minutes and some control over the environment.
The model also demands skilled facilitation. Stage 4 in particular, where the clinician creates space for emotional expression without offering premature reassurance, often runs counter to clinical instinct and training. Educators should therefore teach Roberts’ model through structured simulation and debrief, not through reading alone.
Teaching Roberts’ Model in Healthcare Education
Because the model is inherently interactional, educators should teach it through practice. Role-play and simulation scenarios are the strongest contexts, especially when they involve acute distress, lethality assessment, and emotionally charged de-escalation. Post-scenario debrief should focus on Stage 2, where rapport is built under pressure; Stage 4, where emotion is validated; and the shift from Stage 5 to Stage 6, where exploration becomes commitment. These are often the points where application breaks down.
Video recording of simulated crisis encounters is particularly valuable here. The micro-behaviours that shape rapport, including tone of voice, pace, body language, and the management of silence, are often invisible to clinicians during the encounter. On playback, they become much easier to observe. Reviewing a recording before debrief gives both facilitator and learner a shared account of what happened. It also grounds discussion of Stages 2 and 4 in specific moments, rather than general impressions.
Conclusion
Roberts’ Seven-Stage Crisis Intervention Model remains one of the most clinically complete frameworks for acute crisis work in healthcare. Its sequenced structure helps prevent common errors in unstructured crisis encounters, including premature problem-solving, inadequate risk assessment, and absent follow-up. Its emphasis on collaboration, from the first moments of rapport-building to the final follow-up agreement, reflects what makes crisis intervention effective.
Healthcare educators teach the model most effectively through simulation, structured debrief, and, where possible, video review of the learner’s own performance. Knowing the seven stages is not enough. Applying them under pressure requires practice, reflection, and feedback.
Related posts: How to Calm and Reassure an Anxious Patient · The SPIKES Communication Model · Effective Debriefing for Simulation-Based Medical Education