
Patient anxiety is a common challenge in healthcare settings. Whether someone is awaiting test results, facing a medical procedure, or navigating a new diagnosis, anxiety can cloud communication, delay care, and reduce overall satisfaction. In high-stress moments (like emergency room visits, invasive treatments, or critical care discussions) even routine interactions can feel overwhelming for patients.
Anxious patients may show it outwardly through restlessness or tears, or quietly through avoidance, shallow breathing, or clinging to brief answers. Recognizing and managing these reactions quickly isn’t just about bedside manner, it’s about clinical effectiveness. When patients feel heard and reassured, they are more likely to follow care plans, understand instructions, and return for follow-ups.
Research supports this. Structured protocols like the SPIKES model, designed for delivering serious news, emphasize empathy and shared understanding as key components of effective communication. Similarly, Roberts’ the Crisis Intervention Handbook highlights how timely emotional support can stabilize patients and improve outcomes, especially in moments of acute stress.
With the right approach, even tense situations can become manageable for both clinicians and patients. In the following sections, we’ll explore techniques that can help reduce anxiety and build trust, tools every care provider should have on hand.
Understanding Patient Anxiety
Not all anxiety is the same, and distinguishing between clinical anxiety and situational anxiety helps guide how to support a patient effectively. Clinical anxiety refers to persistent, excessive worry that interferes with daily life. It’s usually diagnosed as an anxiety disorder like GAD (Generalized Anxiety Disorder) or panic disorder, often requiring long-term management and possibly medication. In contrast, situational anxiety is short-term and triggered by specific circumstances—such as a hospital visit, medical procedure, or bad news.
Recognizing which type you’re dealing with is essential when it comes to calming and reassuring an anxious patient, as it guides the appropriate communication and support. These may include rapid breathing, restlessness, irritability, dry mouth, sweating, shaking, or even freezing up. Patients may avoid eye contact, seem overwhelmed, or ask the same question repeatedly. Physiological responses—like elevated heart rate or nausea—are common. Clinicians may also notice indecisiveness or difficulty articulating concerns.
Anxiety affects communication in a few key ways. First, it shortens attention span, making it harder for patients to absorb details or instructions. Emotional arousal also shifts the brain away from logical processing toward survival responses. That can lead to confusion, poor decision-making, or mistrust of clinical guidance. In high-stress moments, even routine interactions can feel threatening to the patient, reducing cooperation and increasing emotional reactivity.
The Psychology of Reassurance
When calming and reassuring an anxious patient, understanding the psychology behind reassurance is essential. Effective communication isn’t just about words—it’s about how those words are delivered, how patients are emotionally supported, and how their sense of control is preserved. Two widely respected models in medical communication, the SPIKES protocol and Roberts’ Crisis Intervention model, offer a helpful framework.
Communication Models in Action
SPIKES Model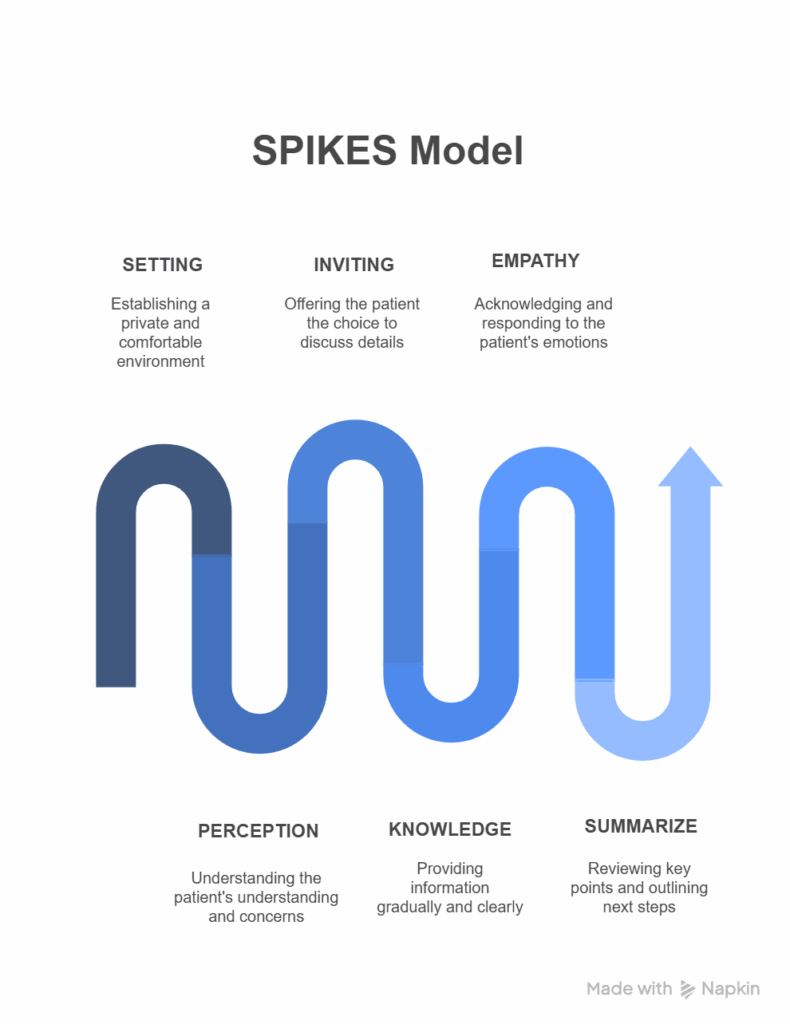
SPIKES, originally developed to guide difficult conversations in oncology, breaks down patient interaction into six steps: Setting up the conversation, assessing the patient’s Perception, obtaining the Invitation to share information, giving Knowledge, addressing Emotions with empathy, and Summarizing with a strategy. Even outside cancer care, SPIKES reinforces how empathy and structure support clinicians in calming and reassuring an anxious patient effectively.
- Setting – Create privacy and eliminate distractions. Sit down, maintain a calm tone, and ensure the patient feels physically and emotionally safe.
- Perception – Ask what the patient understands about the situation so far. Let them explain in their own words.
- Invitation – Gauge how much detail they want. Some anxious patients may prefer simple, high-level information at first.
- Knowledge – Explain what’s happening in clear, non-technical language. Use analogies if needed.
- Empathy – Acknowledge emotions directly. Phrases like “It makes sense that you’re feeling this way” validate their experience.
- Strategy & Summary – Outline what’s next and ensure they know they’re not facing it alone. Reconfirm availability and next steps.
When applied in this context, SPIKES becomes more than a disclosure framework—it’s a tool for anchoring patients in clarity and trust. It’s been recommended in clinical training for high-stress care environments, including emergency and critical care settings. For a more indepth dive into the SPIKES model, check out this blog.
Roberts’ 7-Stage Crisis Intervention Model
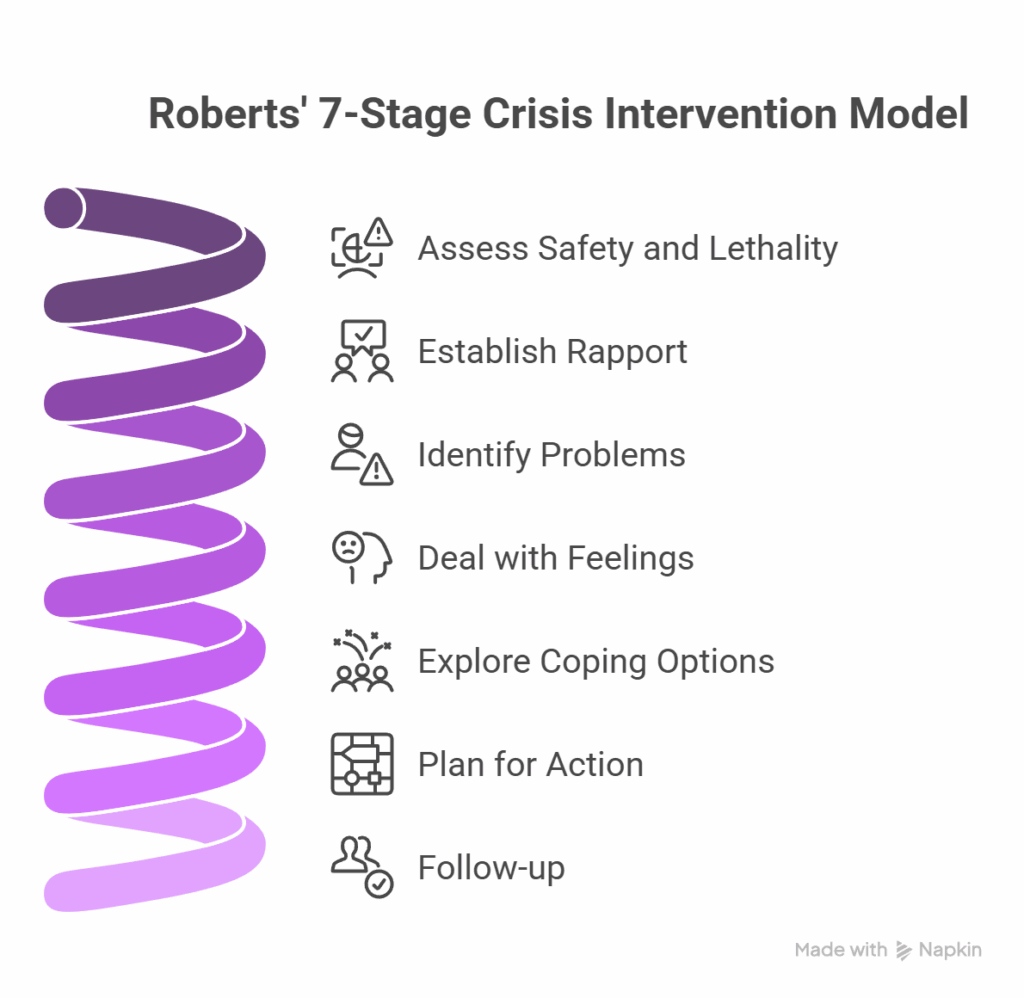
Developed by Dr. Albert Roberts, this model breaks down crisis de-escalation into actionable steps. Through its seven-stages it emphasizes building rapport, validating emotions, exploring coping skills, and collaboratively forming an action plan. Although typically used for acute psychiatric crises, it’s highly effective for managing anxiety in medical or therapeutic settings.
-
Assess safety and lethality – Quickly identify if the patient is at risk of harm to self or others. If not, move to emotional assessment.
-
Establish rapport – Use open body language and reflective listening. Avoid interrupting. Rapport builds faster when patients don’t feel judged.
-
Identify problems – Ask what triggered their anxiety today. Clarify if it’s related to pain, diagnosis, isolation, or other factors.
-
Deal with feelings – Let the patient express emotions freely. Normalize their experience with gentle prompts like, “A lot of people feel this way here.”
-
Explore coping options – Collaborate on what’s worked for them in the past and suggest short, immediate calming techniques like paced breathing.
-
Plan for action – Propose a clear plan: it could be speaking with a nurse regularly, getting reassurance before each procedure, or having a loved one present.
-
Follow-up – Recheck later that day or during the next visit. Consistency strengthens trust.
Empathy helps patients feel understood, which reduces perceived threat. When patients are treated as active participants—offered clear options and space to speak—they regain a sense of control. Emotional safety builds when patients aren’t rushed, judged, or silenced.
Why communication changes the patient’s emotional state
In healthcare settings, anxiety is not only shaped by symptoms or diagnosis. It is also strongly influenced by communication. Patients often become more distressed when they do not understand what is happening, how long they will wait, or what the next step will be.
Recent NHS England qualitative analysis of urgent and emergency care experiences found that uncertainty, poor expectation management, and inconsistent communication significantly increased stress during care experiences. Patients repeatedly linked reassurance to simple but consistent behaviors such as being listened to, receiving updates, and having procedures clearly explained.
The report identified “trust and confidence” as a central factor in patient experience, particularly during periods of waiting and uncertainty. Patients described feeling calmer when staff communicated clearly, explained delays honestly, and acknowledged emotional concerns rather than focusing only on clinical tasks.
Several patient accounts specifically highlighted the calming effect of supportive communication:
“The A&E staff were so good at informing me, especially as was very nervous – Broken wrist, they were all very good and helped me stay calm and explained everything.”
Other responses showed the opposite pattern. Anxiety often escalated when patients felt ignored, dismissed, or left without updates for long periods. NHS England’s analysis noted that lack of communication around waiting times created additional stress and frustration, especially in already vulnerable patients.
This reflects an important principle in patient-centered communication: reassurance does not come primarily from saying “don’t worry.” It comes from reducing uncertainty. Clear explanations, active listening, emotional acknowledgment, and predictable next steps help patients regain a sense of orientation and safety during care interactions.
7 Evidence-Based Techniques to Calm and Reassure Patients
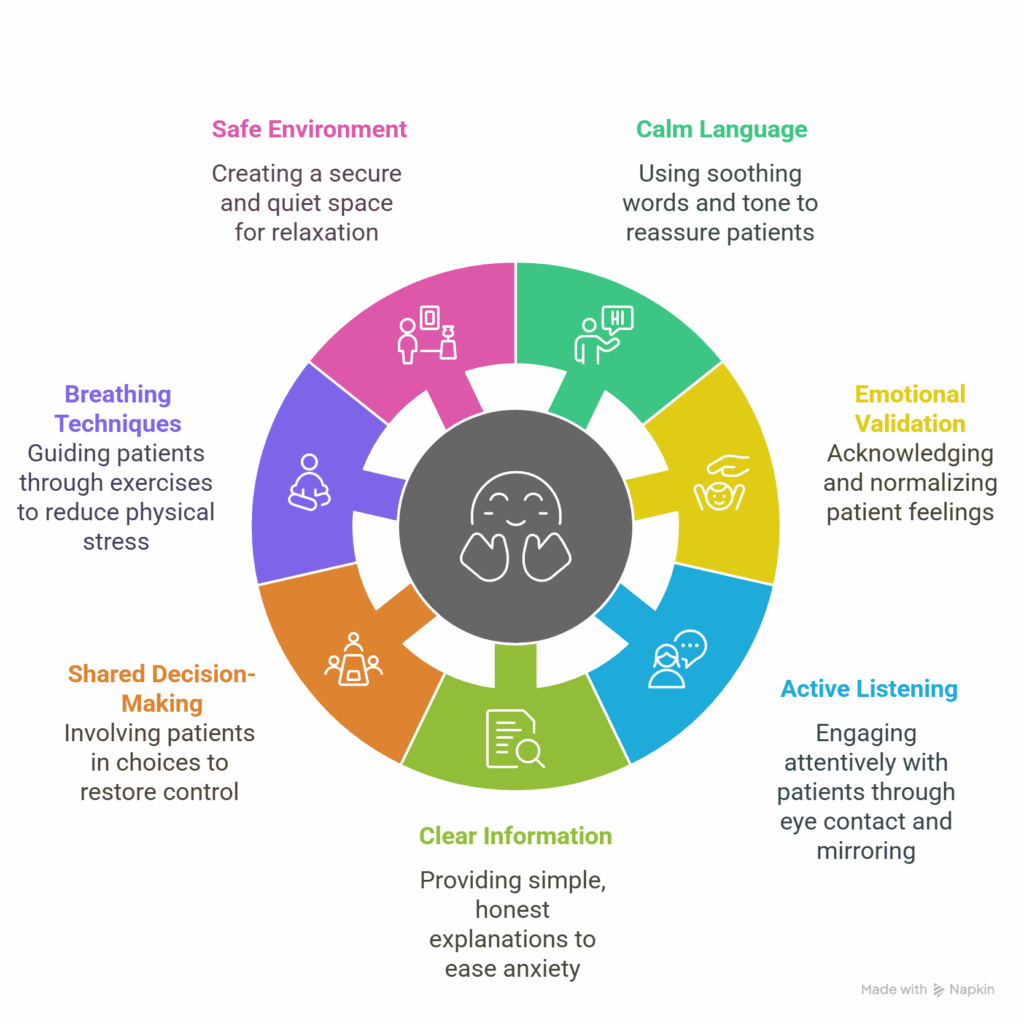
1. Use Calm, Reassuring Language
Tone sets the stage. Speak slowly and clearly, using simple words. Avoid medical jargon unless it’s explained. Phrases like “You’re safe here” or “We’ll go one step at a time” can reduce distress quickly. Even the way a provider greets someone matters—being warm and present helps anchor the patient. Calm language shapes how patients perceive their safety and care
2. Acknowledge and Normalize Their Emotions
Let patients know their anxiety is valid. Avoid dismissing or minimizing their fears. Say things like “It’s completely okay to feel nervous about this” to show you’re listening. Recognizing anxiety without trying to ‘fix it’ immediately builds rapport. As noted by Hopkins Medicine, emotional validation often lowers physical signs of stress.
3. Practice Active Listening and Eye Contact
Patients are quick to pick up on where your focus lies. Put away distractions, make steady eye contact, and mirror their emotions with attentive body language. Reflecting or paraphrasing what they say shows you’re listening, not just hearing. These nonverbal cues build trust rapidly. This blog on nonverbal communication in healthcare highlights how eye contact and posture directly impact patient comfort and reduce anxiety during medical interactions.
4. Provide Clear, Honest Information
Clarity eases anxiety. When patients don’t understand what’s happening, their stress increases. Break information into small, manageable chunks and avoid overloading them. Use simple language, and follow up by asking if anything needs repeating. Visual aids, like diagrams or written instructions, can reinforce verbal communication. When discussing outcomes, stay honest but compassionate. Phrases like “We’ll handle this together” can balance honesty with emotional reassurance.
5. Involve the Patient in Decision-Making
Shared decision-making helps restore a sense of control. Offer choices when possible—whether it’s picking a time for a procedure or deciding on a treatment path. Studies have shown that the act of collaboration reduces emotional tension and increases satisfaction with care.
6. Offer Breathing or Grounding Techniques
Guided breathing and grounding can quickly reduce physiological symptoms of anxiety like rapid heartbeat, dizziness, or chest tightness. A simple breathing exercise involves inhaling slowly through the nose for four seconds, holding for four, and exhaling through the mouth for six. This activates the parasympathetic nervous system and helps calm the body.
Grounding techniques work by shifting focus away from internal anxiety and toward the external environment. One popular method is the 5-4-3-2-1 technique: patients are asked to name five things they can see, four they can touch, three they can hear, two they can smell, and one they can taste. This engages the senses and reduces spiraling thoughts.
7. Create a Safe, Quiet Environment
Anxiety often escalates in chaotic or overstimulating spaces. Make the setting feel secure by reducing noise, dimming harsh lighting (when possible), and maintaining physical boundaries like closed doors or privacy curtains. Creating a stable, sensory-controlled space plays a key role in calming and reassuring an anxious patient, especially in unfamiliar settings.
Mistakes to Avoid When Reassuring Anxious Patients
When trying to calm and reassure an anxious patient, good intentions can backfire if not handled with care. One common mistake is overpromising. Saying “everything will be fine” may sound comforting, but it can undermine trust if outcomes are uncertain. Instead, offer realistic support and focus on what can be done now.
Another frequent error is ignoring or minimizing the patient’s concerns. Phrases like “don’t worry” or “you’re overthinking it” can feel dismissive and increase distress. Acknowledging their emotions shows empathy and builds rapport.
Rushing the conversation or using medical jargon is also counterproductive. It creates confusion, increases anxiety, and makes patients feel unheard. Slow down and explain clearly in everyday language.
These missteps are easy to make, especially in high-pressure settings, but being mindful helps reduce them.
Conclusion
Calming and reassuring an anxious patient isn’t about having the perfect words—it’s about presence, clarity, and connection. Anxiety can cloud decision-making, interrupt care, and erode trust. But with simple, consistent strategies—like listening actively, explaining clearly, and validating emotions—you can help patients feel safe, understood, and involved.
Tools like the SPIKES model and Roberts’ Crisis Intervention framework aren’t just for extreme situations. They’re practical blueprints for improving everyday communication, especially in high-stress moments. When you respond with empathy and structure, patients are more likely to engage, follow through on care, and return for follow-ups.
Healthcare is full of uncertainty, but reassurance is something you can control. And sometimes, the calm you offer becomes the difference between fear and trust.
For more strategies on emotionally intelligent communication, visit our blog on patient-centered care.
Frequently asked questions
How do you calm an anxious patient before a procedure?
Start by acknowledging the anxiety directly rather than minimising it. Phrases like “it makes sense that you are feeling nervous” signal that you are listening. From there, a brief explanation of what will happen and what the patient will feel reduces anticipatory anxiety more reliably than general reassurance. Non-verbal cues matter equally here — see our guide on mirroring body language in clinical consultations for practical techniques you can use from the first moment of contact.
What causes anxiety in patients during clinical consultations?
Patient anxiety usually comes from uncertainty, loss of control, or previous negative experiences with healthcare. The clinical environment itself often contributes, including unfamiliar equipment, formal terminology, and time pressure that makes patients feel like a burden. Clinicians who slow their pace and use plain language consistently report more cooperative and less distressed patients.
Does patient anxiety affect clinical outcomes?
Yes, and the evidence is well established. Anxious patients are less likely to recall post-consultation instructions, less likely to adhere to treatment plans, and more likely to experience heightened pain perception during procedures. Addressing anxiety is therefore not only a communication skill but a clinical one with direct downstream effects on care quality.
What is the difference between reassurance and empathy in patient communication?
Reassurance tells a patient that everything will be fine. Empathy acknowledges what they are feeling without making a prediction about the outcome. Research consistently shows that empathy is more effective than reassurance in reducing patient distress, partly because patients often sense when reassurance is not grounded in their specific situation. When a consultation involves visible patient distress, the techniques covered in de-escalation in healthcare complement the empathy-first approach well.
How does non-verbal communication help calm an anxious patient?
Non-verbal cues often carry more weight than spoken words in high-anxiety situations. Maintaining eye contact, adopting an open and relaxed posture, and matching the patient’s pace of speech all signal safety and attentiveness. Sitting down rather than standing, when possible, has been shown to increase patient perceptions of time spent with them, even when the consultation length is identical.
How do you identify when a patient is anxious but not saying so?
Patients frequently mask anxiety with brevity, deflection, or overcooperation. The signs are usually physical: shallow breathing, reduced eye contact, clipped sentences, or a slight increase in vocal pitch. Developing the ability to read these signals accurately is a trainable skill. Our post on identifying emotional cues during a consultation covers the specific behaviours to watch for and how to respond to each one.