

Feedback after clinical observation is one of the most powerful tools in medical education – but only when it’s structured well. Without a framework, post-consultation debriefs tend to drift toward the supervisor’s priorities, skip what the learner actually needs, or stall at vague praise. Pendleton’s Rules were designed to prevent exactly that.
Originally proposed in David Pendleton’s landmark work The Consultation (Pendleton et al., 1984), the model emerged from a study of GP consultations in the UK. The research team found that post-consultation feedback was often poorly structured, heavily negative, and observer-led rather than learner-centered. Their response was a simple, sequenced approach that put the learner first.
Four decades later, Pendleton’s Rules remain one of the most widely used feedback frameworks in clinical education – taught in medical schools, applied in OSCE debriefs, and referenced in healthcare communication training worldwide.
What Are Pendleton’s Rules?
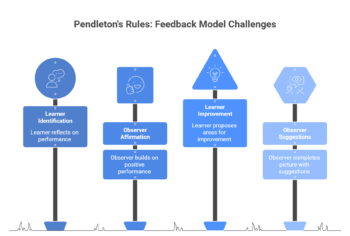
Pendleton’s Rules is a four-step structured feedback model:
- The learner identifies what went well – before the observer says anything, the learner reflects on what they did effectively
- The observer adds what went well – the observer builds on and affirms positive performance
- The learner identifies what could be done differently – the learner proposes areas for improvement in their own words
- The observer adds what could be done differently – the observer completes the picture with their own suggestions
The sequence is deliberate. Asking the learner to speak first prevents the observer from dominating. Opening with positives lowers psychological defensiveness and creates a more receptive climate for critique. And asking what could be done differently rather than what went wrong frames improvement as forward-looking rather than remedial.
It sounds simple. In practice, it changes the dynamic of a feedback conversation significantly.
Why the Sequence Matters
The core insight behind Pendleton’s Rules is that learners process feedback better when they are active participants rather than passive recipients. Research in educational psychology consistently shows that self-generated feedback, where learners identify their own gaps, is retained more deeply and acted on more readily than feedback delivered top-down (Hattie & Timperley, 2007). Branch and Paranjape (2002) make a related point in their influential overview of feedback in clinical education: reflection and feedback are mutually reinforcing, and feedback conversations that prompt self-assessment activate the same reflective processes that consolidate learning outside the feedback session itself.
The positive-first rule also has a clear research basis. High-stakes clinical environments make learners vigilant and defensive. Starting with strengths is not a politeness convention – it signals that the observer genuinely noticed what worked, which makes subsequent critique feel balanced rather than cumulative. Morris’s (2021) systematic review of formative assessment and feedback identifies learner agency – the degree to which learners feel they have ownership of the improvement process – as one of the two key conditions for feedback to produce behavior change. Pendleton’s Rules are structured precisely to create that agency from the first question.
The model also carries an implicit professional message: patient-centered communication requires the clinician to listen before advising. Structuring feedback the same way reinforces the principle through practice.
How it’s used in clinical education today
Pendleton’s Rules are most commonly applied in three settings:
- OSCE feedback sessions. After a simulated patient encounter, examiners guide students through the four steps. The learner identifies strengths first, which often reveals gaps in self-awareness. Students who over-criticise themselves can see an examiner confirm what they did well. Students who missed a key issue get a structured chance to recognise it before the examiner points it out.
- GP and primary care consultation review. The model was designed for this context. Supervisors watching trainees conduct real consultations use Pendleton’s structure to debrief without dominating. It is especially useful where the power differential between trainer and trainee is large, and where direct criticism could damage the learning relationship.
- Communication skills training. When students practice breaking bad news, conducting difficult conversations, or managing anxious patients, Pendleton’s Rules provide a reliable structure for both peer and supervisor feedback. Students reviewing each other’s recorded consultations use the four-step sequence to keep the debrief focused and constructive.
Video review adds a layer that Pendleton himself could not have anticipated in 1984. When learners watch a recording of their own consultation before the debrief, they arrive with specific observations rather than general impressions, which makes step one far more precise and genuinely reflective than memory alone allows. Perron et al. (2016) found that video-based feedback in formative OSCEs produced equivalent learning outcomes to direct observation, with the added advantage that learners could review specific moments rather than relying on an observer’s summary. Dohms et al. (2020) extended this in a study using recordings of real GP consultations, finding that video feedback measurably improved communication skills compared to verbal feedback alone.
Strengths and Limitations
Strengths
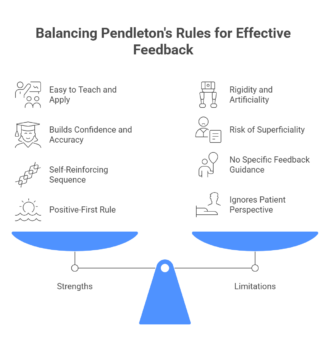
Pendleton’s Rules are easy to teach, easy to remember, and easy to apply under time pressure. The sequence is self-reinforcing: once a learner has experienced it from both sides, they begin to apply the same structure to their own self-reflection.
The positive-first rule is particularly valuable in early training. Medical students and junior clinicians often struggle to recognize what they’re doing well. Structuring the conversation to start there builds both confidence and observational accuracy, which are prerequisites for honest self-assessment.
Limitations
The model’s most cited weakness is rigidity. Requiring positives before negatives can feel artificial, particularly in situations where something went seriously wrong and both parties already know it. Some educators find the sequence stilted, especially in repeated use with the same learner over time.
The model also risks becoming superficial. Observers can reduce “what went well” to a box-ticking exercise if they do not engage seriously. Pendleton’s Rules also tell educators when to give critical feedback, but not how to deliver it well. The structure exists, but educators still need to develop the skill.
A further critique is that the original model doesn’t explicitly ask about the patient’s perspective or outcomes. Later revisions, sometimes called Modified Pendleton’s, address this by adding a prompt: “What do you think the patient was experiencing?”
How Pendleton’s compares to other feedback models
Pendleton’s Rules sit alongside several other structured feedback approaches used in clinical education.
- The feedback sandwich (praise–critique–praise) is superficially similar but consistently less effective. Sandwiching criticism between two positives tends to dilute the message – learners remember the praise and filter out the critique. Pendleton’s Rules separate the positive and critical phases clearly, which helps both land.
- SET-GO (Share, Elaborate, Transfer – Goals, Options) is a more conversational approach that moves entirely away from the observer’s perspective, asking the learner to set their own goals. It suits experienced practitioners who want self-directed development better than students who still need external structure.
- Agenda-Led Outcomes-Based Analysis (ALOBA), developed at the University of Calgary, starts from what the learner was trying to achieve rather than what the observer noticed. It is more flexible but also more demanding to facilitate well.
- Pendleton’s sits in the middle of this spectrum: more structured than ALOBA, less mechanical than the sandwich, and better suited to early-stage learners than SET-GO. The choice between models often comes down to the learner’s experience level and the available time.
Using Pendleton’s Rules with video review
One of the most effective applications of Pendleton’s Rules is pairing the four-step debrief with a video recording of the consultation. Video changes what’s available in step one. The learner watches the interaction back before the debrief instead of relying on memory, so they ground their self-assessment in what actually happened rather than how it felt.
Platforms like Videolab allow learners to annotate specific moments in a recording before meeting with their supervisor. They can mark moments where communication felt strong and flag moments of uncertainty, giving both parties a shared, concrete reference point for the Pendleton conversation.
This combination (structured reflection model plus recorded evidence) is particularly effective for communication behaviors that are invisible in the moment but clearly visible on playback: body language, pacing, silence, and the micro-expressions that patients respond to but clinicians rarely notice while they’re happening.
Conclusion
Pendleton’s Rules remain relevant because the problem they solve remains relevant: feedback in clinical education tends to be unstructured, observer-led, and poorly retained. The model’s four-step sequence – learner first, positives first, forward-facing critique – addresses all three.
Its limitations are real. Rigid application can feel formulaic, and the model offers no guidance on how to give critical feedback, only when. But as a starting framework for clinical supervisors and as a structure for teaching learners how to receive feedback, it holds up well across settings and experience levels.
For programs using video-based feedback, Pendleton’s Rules provide a natural complement: a structured debrief around recorded evidence, with the learner’s reflection anchored in what they can see rather than what they remember.
Related posts: Formative vs Summative Feedback · Implementing Feedback Models in Healthcare Education · Peer Feedback in Medical Education