

A useful simulation scenario does not begin with a dramatic patient history. It begins with a performance problem. What should learners be able to notice, decide, say, or do differently after the session?
This distinction matters because an elaborate case can still produce unfocused learning. Conversely, a relatively simple patient encounter can expose how learners gather information, communicate under pressure, divide responsibilities, and respond to feedback.
The six medical simulation scenarios below illustrate different educational purposes. Each can be adapted to the learner level, clinical discipline, available modality, and local protocols. After the examples, a practical checklist shows how to turn a learning need into a scenario that facilitators can run consistently.
What is a medical simulation scenario?
A medical simulation scenario is a planned representation of a clinical event designed around specific learning or assessment objectives. It defines the participants, patient context, starting information, expected actions, cues, progression, endpoint, and debriefing plan.
The scenario is only one part of the learning experience. The Healthcare Simulation Standards of Best Practice place scenario design within a wider process that includes a needs assessment, objectives, preparation, prebriefing, facilitation, debriefing, evaluation, and pilot testing. Therefore, educators should not treat a patient script as a complete simulation plan.
Medical simulation scenarios can address technical skills, clinical reasoning, teamwork, communication, leadership, or combinations of these outcomes. The appropriate modality follows from the objective. A simulated patient may be better than a manikin for a difficult conversation, while an in situ team scenario may be appropriate when the learning need concerns roles, equipment, or workflow.
Six medical simulation scenarios for healthcare education
Strong scenarios create observable decisions and behaviors that can be discussed or assessed. The following examples describe the educational structure rather than prescribing clinical management. Educators should align all clinical details with current local guidance and involve a subject matter expert.
1. Recognizing and escalating patient deterioration
This scenario tests whether learners can identify a meaningful change, prioritize an initial response, and escalate concerns clearly. It suits medical, nursing, paramedic, and interprofessional groups at different stages of training.
The patient begins in an apparently stable state but presents several cues that become more concerning over time. The facilitator releases observations, examination findings, or new information according to the learners’ actions. The case should not depend on one obscure diagnosis. Instead, its central challenge is recognizing the pattern, reassessing the patient, and communicating the level of concern.
Observable behaviors might include gathering relevant information, calling for help, using a structured escalation format, allocating roles, and communicating with the patient. The endpoint could be an appropriate escalation decision rather than a fully resolved clinical case.
During debriefing, the facilitator can examine which cues changed the team’s interpretation, what delayed escalation, and how information moved between participants. This keeps the discussion focused on reasoning and teamwork instead of turning it into a test of diagnostic recall.
2. Conducting a safe clinical handover
This scenario makes the quality of information transfer visible. It works well when learners know a handover framework in theory but struggle to select, organize, and verify information during practice.
One participant receives a patient record containing relevant details, distracting details, and one unresolved risk. Another participant assumes responsibility for the patient. Time pressure can be introduced, but it should not be so severe that it overwhelms the intended communication objective.
The receiving clinician should have an active role. Expected behaviors can include asking clarifying questions, checking responsibility for outstanding actions, and confirming the immediate plan. This avoids framing handover as a one way presentation.
A video recording can help participants review information selection, sequencing, interruptions, and closed loop confirmation. If video is used, the prebrief should explain who can access the recording, how it will be used, and when it will be deleted. The recording should support a defined learning purpose, not become a substitute for skilled facilitation.
3. Responding to an upset patient or relative
This simulated patient scenario develops communication under emotional pressure. The objective is not to produce a perfect script. It is to help learners notice emotion, listen, explain boundaries or uncertainty clearly, and agree on an appropriate next step.
The scenario might involve a delayed appointment, an unexpected change in care, conflicting expectations, or concern about a perceived error. The simulated patient’s emotional response should be calibrated to the learner level and linked to the purpose of the session. Escalating anger without an educational reason can turn the exercise into endurance rather than learning.
Useful observable behaviors include acknowledging the concern, avoiding premature reassurance, asking focused questions, checking understanding, and summarizing the agreed action. The simulated patient can also provide feedback on how the interaction felt, provided they have been trained and supported for that role.
This scenario can connect with teaching on calming and reassuring an anxious patient. However, the scenario objectives should remain narrow enough for participants and observers to identify specific evidence of performance.
4. Resolving a medication discrepancy
This scenario examines how learners manage incomplete or conflicting information before it reaches the patient. It can combine clinical reasoning, speaking up, documentation, and interprofessional communication without requiring an emergency.
The patient record, medication list, verbal handover, or available medication contains a discrepancy. Learners must notice the inconsistency, determine what needs verification, and communicate with the relevant person. The facilitator should define which information is available on request and how the environment responds to appropriate action.
The case can be adapted to different professions. For novice learners, the discrepancy and communication route may be relatively clear. More experienced participants might face competing explanations, interruptions, or unclear ownership. Any added difficulty should test the stated objectives rather than reward guessing.
The debrief can explore the difference between individual vigilance and system conditions. It can also examine whether hierarchy, assumptions, or ambiguous responsibility affected the response.
5. Coordinating an interprofessional discharge
This scenario reveals whether a team can create a shared, patient centered plan across professional boundaries. It suits learners from medicine, nursing, pharmacy, physiotherapy, occupational therapy, and other health professions.
Each participant receives information relevant to their role, while no single person initially holds the complete picture. The patient has priorities or constraints that may not align neatly with the team’s first plan. Participants must exchange information, clarify roles, involve the patient, and identify unresolved risks.
Role authenticity is important. Participants should normally perform within a role they understand, with enough orientation to contribute meaningfully. Research on interprofessional simulation indicates that learners’ perceptions of realism can differ by profession, so design decisions should consider how each group can enact its expected contribution rather than merely appear in the room.
The debrief can focus on how the team formed a shared plan, whose information shaped the decision, and whether the patient perspective changed the outcome. Further examples of team behaviors are available in Videolab’s guide to interprofessional collaboration in healthcare.
6. Giving feedback after an observed clinical task
This scenario allows clinical educators and supervisors to practice feedback as an observable professional skill. One participant completes or watches a short clinical task, then another conducts the feedback conversation.
The challenge may involve a learner who is disappointed, defensive, overly self critical, or unaware of a specific performance gap. The feedback provider must create a focused conversation, use observable evidence, invite the learner’s perspective, and agree on a realistic next step.
The scenario can be run with a simulated learner or through structured role play. Video can make conversational patterns available for review, including the balance of speaking time, the specificity of evidence, and the point at which the learner disengages or begins to reflect.
This example is particularly useful for faculty development because it separates feedback knowledge from feedback performance. Educators can compare the purpose of the exercise with the distinctions between formative and summative feedback before deciding how the interaction should be framed.
How to design a medical simulation scenario
Scenario design should follow a transparent sequence from learning need to observable outcome. The TEACH Sim framework and the Healthcare Simulation Standards both support systematic planning rather than beginning with equipment or dramatic case details.
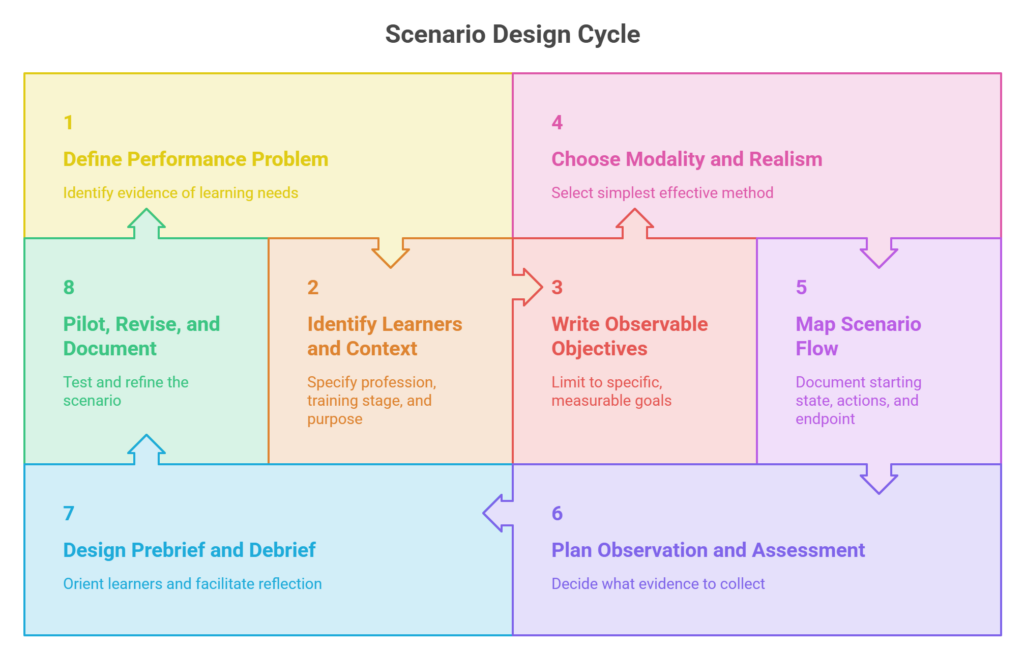
1. Define the performance problem
Start with evidence of a learning, practice, or system need. This might come from curriculum mapping, assessment results, learner feedback, incident review, a new protocol, or observation of clinical work.
Write the problem in behavioral terms. “Learners need more confidence” is difficult to design around. “Learners do not consistently escalate a deteriorating patient using the required information” gives the scenario a clearer purpose.
2. Identify the learners and context
Specify profession, training stage, prior experience, group composition, and prerequisites. A scenario appropriate for final year students may be unsafe or unproductive for novices. Likewise, an interprofessional scenario requires meaningful work for every participating profession.
Decide whether the scenario is educational or assessive. Learners should know which purpose applies because it affects preparation, psychological safety, expected difficulty, and how performance information will be used.
3. Write a small set of observable objectives
Limit the scenario to a manageable set of objectives that describe what learners should demonstrate. Each objective should be specific enough to guide the scenario, observation, and debriefing.
For example, “understand handover” is not directly observable. “Deliver a structured handover that identifies the immediate risk and outstanding action” gives facilitators and learners clearer evidence to examine.
4. Choose the modality and level of realism
Select the simplest modality that can generate the required behavior. Physical realism is only one design consideration. The roles, decisions, time pressure, interpersonal dynamics, and consequences must also feel credible to the participants.
A simulated patient may be appropriate for communication objectives. A task trainer may suit a procedural objective. A manikin can support patient deterioration, while role play or screen based cases may be sufficient for handover and clinical reasoning. In situ simulation is most useful when the actual environment, team, equipment, or workflow forms part of the learning need.
5. Map the scenario flow, cues, and branches
Document the starting state, available information, expected actions, patient or team responses, changes over time, and endpoint. Then identify where learners might take an unexpected path.
Dieckmann and colleagues describe planned interventions for situations in which a scenario departs from its intended course as scenario life savers. These interventions may operate inside the scenario, such as a patient providing a cue, or outside it, such as a facilitator pausing to clarify a technical limitation. They should protect the learning opportunity without forcing participants through a hidden script.
6. Plan observation and assessment
Decide what evidence observers will collect and how it relates to each objective. Avoid broad judgments such as “good communication” when a more specific behavior can be recorded.
If the scenario supports summative assessment, the blueprint, standard setting process, rater preparation, and evidence of validity require more attention than a teaching scenario. A simulation that works well for discussion does not automatically produce defensible assessment decisions.
7. Design the prebrief and debrief together
The prebrief should orient learners to the environment, equipment, roles, expectations, confidentiality, and purpose of the activity. It should also make clear whether the exercise is formative or summative and how recordings or performance data will be handled.
The debriefing plan should connect directly to the objectives and likely events. Facilitators need prompts that help participants reconstruct what happened, examine their reasoning, and consider alternatives. Videolab’s overview of debriefing models for simulation can help educators select an approach that fits the participants and purpose.
8. Pilot, revise, and document the scenario
Run the scenario before using it with the intended learners. A pilot can reveal missing information, unrealistic timing, equipment problems, ambiguous cues, impossible expectations, and branches that the written plan does not cover.
Document revisions, clinical references, version dates, and ownership. The HEIW scenario quality assurance process offers a useful example of reviewing submissions against defined criteria before adding them to a shared repository.
Medical simulation scenario design checklist
A scenario is ready to pilot when another facilitator can understand its purpose, run its progression, and identify the intended evidence of learning. Use this checklist before delivery:
- The learning or performance need is supported by evidence.
- The target learners, prerequisites, and professional roles are specified.
- The educational or assessment purpose is explicit.
- Each objective describes an observable action or decision.
- The modality and level of realism serve the objectives.
- The patient context avoids unnecessary stereotypes and irrelevant complexity.
- The starting information, cues, progression, branches, and endpoint are documented.
- Expected actions and observation criteria align with the objectives.
- Facilitators have a plan for unexpected learner actions.
- The prebrief covers orientation, expectations, psychological safety, confidentiality, and data use.
- The debriefing plan addresses the objectives and likely performance gaps.
- Clinical content has been checked against current local guidance.
- Equipment, staffing, timing, and technical requirements are feasible.
- The scenario has been piloted and revised.
- The version, authorship, references, and review date are recorded.
Using video within simulation scenarios
Video is most useful when it captures evidence connected to the scenario objectives. In a handover scenario, that evidence might be information selection and confirmation. In a faculty feedback scenario, it might be the use of observable examples and the learner’s response.
Videolab provides a GDPR compliant environment for recording, reviewing, annotating, and assessing video from clinical and professional skills training. Educators can connect comments and rubric criteria to specific moments in a performance, which helps keep review focused on observable behavior. The recording workflow, access permissions, retention period, and educational purpose should be defined before the scenario begins.