

Reflection is widely required in healthcare education. Nursing portfolios, clinical placement reports, CPD logs, and supervision meetings all ask practitioners to reflect on their work. But reflection is harder than it sounds. Without structure, it tends to collapse into either description (“here’s what happened”) or vague self-criticism (“I should have done better”). Neither leads to meaningful change.
Gibbs’ Reflective Cycle, introduced by Graham Gibbs in his 1988 guide Learning by Doing, provides that structure. Its six stages move the practitioner from factual description through emotional acknowledgement, into analysis, and out through concrete planning. Developed originally for teaching professionals, it has become one of the most widely adopted reflective models in nursing, allied health, and clinical education globally.
This guide explains how the model works, how to apply each stage in healthcare contexts, and when it is, and is not, the right tool.
What Is Gibbs’ Reflective Cycle?
Gibbs’ model builds on Kolb’s experiential learning cycle but expands the reflective phase into four distinct sub-stages, making it more accessible for practitioners working through complex or emotionally charged clinical experiences. Where Kolb moves through experience, reflection, conceptualization, and experimentation, Gibbs structures reflection in a way that explicitly includes emotional processing — something clinical practice demands and most reflective models underestimate.
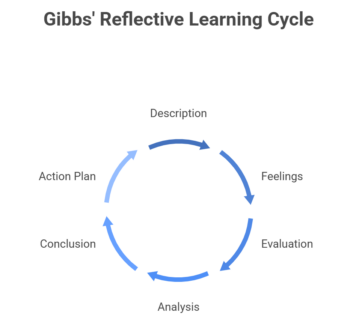
The six stages are:
- Description — What happened? This stage is factual. Who was involved, what was said, what was done. No interpretation yet. The goal is to record the event accurately before analysis colors the memory.
- Feelings — What were you thinking and feeling at the time? This stage invites honest emotional acknowledgement. Clinicians are often trained to set feelings aside, which is partly why reflective writing in healthcare can feel hollow. Acknowledging emotions is not indulgence, it surfaces information about how the experience affected clinical reasoning and behavior.
- Evaluation — What was good and bad about the experience? Here the practitioner begins to assess. Not everything was a failure; not everything was a success. This stage asks for a balanced view, which prepares the ground for honest analysis.
- Analysis — What sense can you make of the situation? This is the intellectually demanding stage. Drawing on theory, evidence, and prior experience, the practitioner asks why things went the way they did. This is where clinical knowledge and reflective insight meet.
- Conclusion — What else could you have done? This stage separates Gibbs’ model from pure introspection. Given what you now understand, what were the alternatives? It is not about blame but about expanding the practitioner’s sense of what was possible.
- Action Plan — If this situation arose again, what would you do? The cycle ends with a commitment to changed behavior, not just changed awareness. Without this stage, reflection risks becoming an intellectual exercise that produces insight without improvement.
The cycle is designed to loop. The action plan feeds back into new experiences, which become the starting point for the next cycle of reflection.
Why Gibbs’ Cycle Matters in Healthcare
Healthcare is a domain where performance errors have direct human consequences, but where the pace of clinical work makes in-the-moment learning difficult. Reflective practice is how experience is converted into professional development: how a difficult consultation becomes a better understanding of breaking bad news, how a near-miss becomes a changed protocol, how a moment of communication breakdown becomes a more considered consultation style.
Donald Schön’s foundational distinction between reflection-in-action (adjusting in real time) and reflection-on-action (reviewing afterward) maps directly onto clinical reality. Gibbs’ Reflective Cycle is primarily a tool for reflection-on-action: a structured way of processing experience after the fact, so that the learning is not lost in the busyness of the next shift.
Research consistently links structured reflective practice to improved clinical performance. A systematic review by Mann, Gordon and MacLeod (2007) found that reflection in healthcare education was associated with improved critical thinking and professional development — though they noted that the quality of facilitation matters significantly. Reflection without structure or feedback can reinforce existing biases rather than challenge them. This is one of the key reasons for using a formal model like Gibbs’ rather than open-ended journaling.
Mamede and Schmidt (2004) go further, demonstrating that structured reflection in medicine is not a single skill but a cluster of distinct cognitive processes and that explicitly structuring the reflective task improves diagnostic accuracy, not just self-awareness. Artioli et al. (2021), drawing on health professionals’ accounts of reflective writing across nursing and medicine, found that the practice supported professional identity formation, increased empathy, and helped practitioners process emotionally difficult encounters — benefits that align directly with the feelings and analysis stages of Gibbs’ model.
Applying the model: A clinical example
A junior doctor leads a family meeting to discuss end-of-life care for an elderly patient. The meeting becomes tense; a family member becomes distressed and asks her to leave. She works through a Gibbs’ reflection:
- Description: I led the meeting. Three family members were present. I presented the palliative care plan using clinical terminology. One family member became increasingly agitated and eventually asked me to stop and leave the room.
- Feelings: I felt unprepared and, at the time, humiliated. I was unsure whether I had made a clinical error or a communication error. I wanted to defend myself but stayed silent.
- Evaluation: The family received accurate information about the clinical situation. However, they did not feel heard or supported. I did not read the emotional state of the room before continuing. My language created distance when the family needed proximity.
- Analysis: Family meetings at end of life require a different communication register than clinical briefings. The family was grieving and managing fear, not processing information. I applied a knowledge-transfer model to a situation that called for empathy first. The SPIKES protocol, which begins by assessing the patient’s and family’s perception and readiness, would have been more appropriate.
- Conclusion: I could have paused earlier and checked how the family was coping. I could have used simpler language and asked what kind of support they needed before presenting a treatment plan.
- Action Plan: Before my next family meeting, I will review the SPIKES framework. I will begin by asking the family what they already understand and what they are hoping to hear, before presenting any clinical information.
This reflection moves from a difficult event to a concrete, behavior-specific plan, which is what distinguishes useful reflection from self-criticism.
How Gibbs’ Cycle is used in healthcare education
Nursing portfolios and placement logs
Most nursing programs require students to submit reflective accounts as part of their assessed portfolio. Gibbs’ cycle is the most commonly taught framework for structuring these accounts, partly because its six stages map naturally onto common assessment criteria: description (evidence of experience), feelings (self-awareness), evaluation and analysis (critical thinking), conclusion and action plan (professional development). Heeneman and Driessen (2017) found that portfolio-based reflection, when properly scaffolded, provided strong evidence of competency development in postgraduate medical training and that the specificity of the framework used was a key determinant of portfolio quality.
Sandars (2009), in his widely cited AMEE Guide to reflection in medical education, reviews Gibbs’, Kolb’s, and Schön’s models side by side and notes that Gibbs’ provides the most accessible entry point for students new to formal reflective practice. Aronson (2010) adds practical guidance for educators: his twelve tips for teaching reflection at all levels of training include using structured models early, then gradually withdrawing the scaffold as learners develop their own reflective habits.
Clinical supervision
In GP training, psychiatry, and many nursing specialties, supervision sessions involve structured reflection on recent clinical encounters. Supervisors familiar with Gibbs’ model use its six stages as a loose agenda, beginning with what happened before asking what the trainee was feeling, then moving toward analysis and planning.
Post-simulation debriefing
Simulation-based education creates controlled clinical experiences specifically designed to be reflected on afterward. Many structured debrief frameworks, including the GAS model (Gather, Analyze, Summarize) and the Diamond debriefing model, share structural similarities with Gibbs’ cycle. When learners use a consistent reflective model across both simulated and real clinical encounters, the habit of structured reflection becomes more deeply embedded.
Continuing Professional Development
Revalidation requirements in nursing, medicine, and allied health typically require evidence of reflection on practice. Gibbs’ cycle provides a widely recognized, assessable structure for meeting these requirements, one that reviewers and appraisers are familiar with, which reduces the friction of the submission process.
Strengths and Limitations
Strengths
Gibbs’ cycle is accessible. Its six stages are clearly labelled and logically sequenced, making it easier to teach and apply than more abstract frameworks like Schön’s. The explicit inclusion of feelings makes it more psychologically complete than purely analytical models — clinical errors and difficult encounters have emotional weight that pure analysis tends to obscure or bypass.
The action plan stage is its most practically valuable feature. It forces reflection to end with a commitment rather than a conclusion, which is the difference between insight and behavior change.
Limitations
The model can produce superficial reflection if used mechanically. Students and trainees sometimes complete each stage as a checklist item rather than a genuine inquiry. The description stage, in particular, can expand into a lengthy narrative that crowds out the analytical stages where most of the learning happens.
Gibbs’ cycle also lacks explicit guidance on incorporating the perspectives of others (patients, families, colleagues) which can be a significant gap in healthcare contexts. Johns’ model of structured reflection (1994) addresses this more directly by asking about external influences, social context, and power dynamics.
The cycle is also primarily retrospective. It does not support the kind of in-the-moment awareness that Schön’s reflection-in-action describes, which is equally important for clinical competence and which Gibbs’ model does not claim to develop.
Gibbs’ vs other reflective models in healthcare
| Model | Stages | Best suited for |
|---|---|---|
| Gibbs (1988) | 6 stages including feelings and action plan | Students, portfolios, emotionally complex experiences |
| Kolb (1984) | 4 stages, more abstract | Conceptual reflection, adult learners |
| Johns (1994) | Structured questions across 5 dimensions | Supervision, experienced practitioners, contextual complexity |
| Driscoll (1994) | 3 questions: What? So what? Now what? | Quick reflection, time-limited settings |
| Schön (1983) | Reflection-in/on-action | Understanding clinical intuition and decision-making |
Gibbs’ sits between Driscoll (too brief for deep reflection on complex events) and Johns (demanding enough to put off beginners). For healthcare students and early trainees, it tends to be the right level of structure — enough to guide genuine reflection without requiring prior experience with formal models.
Using video to support Gibbs’ Reflection
One of the practical challenges of working with Gibbs’ cycle is that memory of a clinical encounter is unreliable. The description stage, which is meant to be factual, is frequently colored by how the experience felt. The feelings stage gets tangled with what actually happened. The evaluation stage reflects what the clinician remembers noticing, not what an observer would have seen.
Video recording of clinical encounters or simulations addresses this directly. When a learner watches a recording before completing their Gibbs’ reflection, the description stage becomes more accurate, the evaluation stage is more grounded in evidence, and the analysis stage has richer and more specific material to work with. Critical moments can be revisited: a pause in communication, a shift in the patient’s body language, a missed cue that only becomes visible on playback. Zhang et al. (2019), in a systematic review of video-assisted debriefing in simulation, found that video-assisted debriefing produced significantly greater improvements in clinical performance and self-efficacy compared to verbal debriefing alone, with effects consistent across nursing, medicine, and allied health contexts.
Platforms like Videolab allow learners to annotate recordings and share them with supervisors ahead of a reflection session. This means the conversation can move immediately into evaluation and analysis rather than spending time reconstructing what happened from memory alone.
For program that require reflective portfolios, video-annotated Gibbs’ reflections also provide stronger evidence of genuine professional development than written accounts alone, the recording demonstrates that the reflection is grounded in a real and specific clinical encounter.
Conclusion
Gibbs’ Reflective Cycle remains one of the most widely used reflective frameworks in healthcare because it solves the right problem: it gives structure to a process that, without it, tends toward description or self-criticism rather than learning. Its six stages guide the practitioner from what happened, through what it meant emotionally and analytically, to what they would do differently.
Its limitations (potential for superficiality, limited attention to others’ perspectives, retrospective scope) are real, and practitioners benefit from using it alongside other approaches as they develop. But as an entry-level framework for students and a portfolio structure for trainees, it remains the most widely accessible and reliably useful reflective model in healthcare education.
The combination of Gibbs’ structure with recorded clinical evidence is where the model becomes most powerful: a framework that turns video review into genuine professional development rather than observation alone.
Related posts: The Importance of Reflective Practice in Healthcare Training · Self-Awareness vs Self-Reflection: Key Differences · Why Metacognition Matters in Medical Education