

What is competency based medical education?
Competency based medical education (CBME) is an approach to training physicians that focuses on the abilities learners must demonstrate in real clinical practice. Instead of measuring progress primarily by the amount of time spent in rotations or courses, CBME evaluates whether trainees can perform key professional tasks safely and effectively.
In traditional medical education, programs often assume that completing a fixed period of training leads to competence. However, CBME reverses this logic. First, educators define the outcomes required for clinical practice. Then curricula, assessments, and learning activities are designed to ensure that trainees achieve those outcomes (Frank et al., 2010).
A competency represents an observable ability that integrates knowledge, skills, and professional attitudes. Because these abilities are observable, educators can measure them through workplace assessments and direct observation (Frank et al., 2010).
As a result, CBME places strong emphasis on performance in authentic clinical environments. Trainees must demonstrate that they can apply clinical reasoning, communicate with patients, and collaborate with healthcare teams before advancing to greater responsibility.
How CBME shifts medical training toward outcomes
One of the defining features of CBME is its focus on outcomes rather than educational process. Instead of asking how long learners should train in a specific environment, CBME asks what abilities graduates must demonstrate to practice safely.
Historically, medical education has relied heavily on time based structures such as rotations and residency duration. Yet this model does not guarantee that every trainee achieves the same level of clinical competence. Consequently, CBME proposes that the goal of training should be clearly defined performance outcomes tied to patient care needs (Frank et al., 2010).
Therefore, competencies become the organizing framework of the curriculum. Programs identify the abilities required of physicians and design learning experiences that help trainees progressively develop those abilities. Because learners develop skills at different speeds, CBME allows for more flexible progression through training stages.
In this framework, educational decisions start with the question: what must physicians be able to do in practice. Curriculum design, teaching strategies, and assessment methods are then aligned with that goal.
Core elements of competency based medical education
Although CBME programs vary across institutions and countries, most share a common structure built around several core elements.
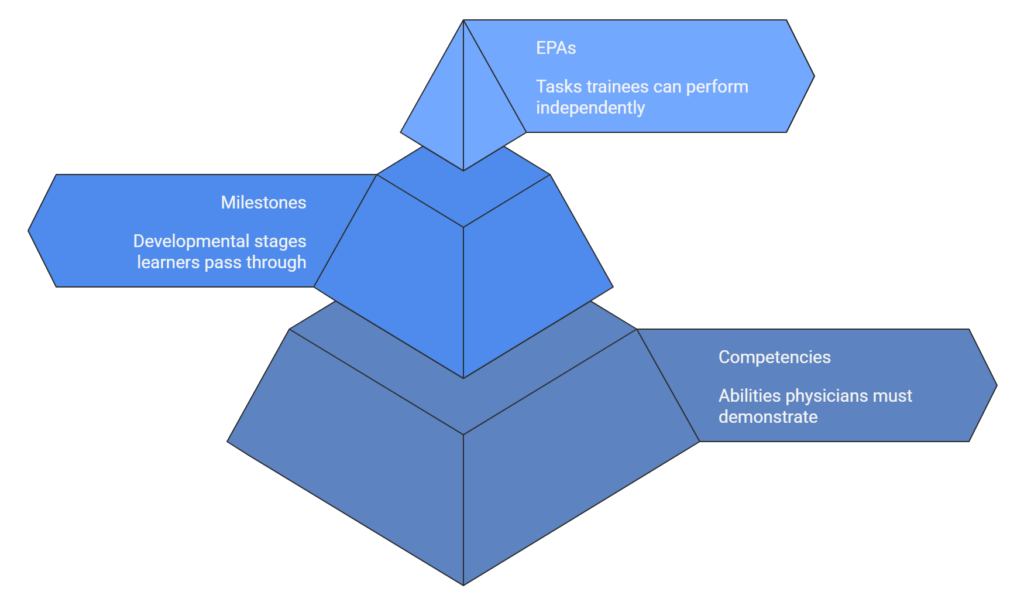
First, competencies define the abilities physicians must demonstrate. These abilities often span multiple domains such as clinical expertise, communication, professionalism, and collaboration.
Second, milestones describe the developmental stages learners pass through as they acquire competence. These milestones provide a roadmap that helps trainees understand what progression looks like throughout training.
Third, Entrustable Professional Activities (EPAs) translate competencies into real clinical work. An EPA represents a task that a trainee can be trusted to perform independently once sufficient competence has been demonstrated (ten Cate, 2005).
Importantly, EPAs are observable activities such as conducting a patient consultation, performing a clinical procedure, or presenting a case during rounds. Because supervisors can directly observe these activities, they provide practical evidence of competence in clinical settings.
How competency based medical education changes assessment
Assessment plays a central role in CBME because progression depends on demonstrated performance rather than time spent in training.
In traditional programs, assessment often occurs through written examinations or periodic evaluations. While these methods measure knowledge, they may not capture how trainees perform in real clinical situations. CBME therefore emphasizes workplace based assessment methods that observe clinical behavior during routine practice.
For example, supervisors may evaluate how trainees communicate with patients, conduct physical examinations, or make clinical decisions. These observations generate evidence of competence across multiple domains of physician performance.
Frequent assessment also supports developmental feedback. Instead of serving only as a final judgment, assessment becomes a continuous learning tool that guides improvement and professional growth. Over time, multiple observations accumulate into a longitudinal record of competence that reflects a trainee’s readiness for independent practice.
Why medical education is moving toward competency based training
Medical education has gradually shifted toward competency based models because traditional training structures cannot always guarantee consistent outcomes. When programs rely primarily on time based rotations, trainees may complete the same curriculum yet graduate with different levels of readiness for clinical practice.
Consequently, educators began to argue that training systems should focus more directly on the abilities physicians must demonstrate in real patient care. Competency based medical education addresses this concern by defining explicit outcomes and aligning education with those outcomes. Frank and colleagues describe CBME as an approach that organizes training around measurable abilities that physicians must demonstrate in practice (Frank et al., 2010).
Patient safety has also influenced the shift toward competency frameworks. Healthcare systems increasingly expect training programs to document that graduates can perform clinical tasks safely and effectively. Competency frameworks allow educators to track whether learners can apply knowledge, communicate with patients, and manage clinical situations in practice.
Furthermore, regulatory organizations and professional bodies have adopted competency frameworks to standardize expectations across training programs. Examples include the CanMEDS framework in Canada and the ACGME competencies in the United States. These frameworks help define the capabilities physicians should demonstrate before practicing independently.
Examples of competencies in medical training
Competencies in medical education represent integrated abilities that combine knowledge, technical skills, and professional attitudes. These competencies reflect the complex responsibilities physicians must manage in real clinical environments.
Clinical expertise is one of the most visible competency domains. Physicians must demonstrate the ability to collect patient histories, perform physical examinations, interpret diagnostic information, and develop appropriate treatment plans.
Communication skills also represent a central competency in healthcare training. Physicians must explain diagnoses, discuss treatment options, and respond to patients’ concerns in ways that promote understanding and trust.
Interprofessional collaboration forms another important competency domain. Modern healthcare relies on teamwork among physicians, nurses, pharmacists, and other professionals. Trainees therefore must learn to coordinate care, share information effectively, and contribute to multidisciplinary decision making.
Professionalism is also frequently included within competency frameworks. Physicians must demonstrate ethical behavior, accountability, respect for patients, and commitment to continuous learning throughout their careers.
Together, these competencies create a structured model for evaluating physician performance across the full range of clinical responsibilities.
Challenges of implementing competency based medical education
Although CBME offers many advantages, implementing this approach introduces several challenges for medical schools and training programs.
One challenge involves the increased need for direct observation. Because CBME requires evidence of clinical performance, educators must observe trainees in real clinical situations more frequently than in traditional training models. This requirement can increase faculty workload and demand new assessment tools.
Another challenge involves assessment consistency. Multiple supervisors often evaluate the same trainee across different clinical settings. Programs must therefore develop structured frameworks to ensure that assessments remain fair and comparable across evaluators.
Tracking competency progression over time can also be complex. Programs must collect evidence from many observations, clinical encounters, and assessments to determine whether trainees have reached expected levels of performance. Touchie and ten Cate note that CBME requires robust systems to gather and interpret assessment data across training environments (Touchie and ten Cate, 2015).
Finally, faculty development plays an essential role in successful CBME implementation. Educators must learn how to observe clinical behavior, provide meaningful feedback, and interpret competency frameworks in everyday clinical teaching.
How video observation can support competency based medical education
Because CBME relies heavily on direct observation of clinical performance, educators increasingly explore technologies that help capture and review clinical encounters. Video recording offers one approach to strengthening observation and feedback within competency based training.
Video allows supervisors to analyze clinical interactions in greater detail than real time observation alone. For example, educators can review how trainees communicate with patients, structure consultations, and respond to emotional cues. These recordings can also support reflective learning by allowing trainees to analyze their own performance.
Furthermore, video documentation can create longitudinal evidence of competency development. When clinical encounters are recorded across multiple training stages, educators can observe how trainees’ skills evolve over time.
Structured evaluation tools can also be applied to recorded consultations. Supervisors may review the same encounter independently and compare their assessments. This process helps improve reliability in competency evaluation.
Video analysis therefore supports several core principles of CBME, including direct observation, feedback, and documentation of professional abilities in real clinical contexts.
How CBME connects to Entrustable Professional Activities
Entrustable Professional Activities represent one of the most practical mechanisms for implementing CBME in clinical training. Instead of assessing isolated skills, EPAs evaluate whether a trainee can perform meaningful professional tasks.
Ten Cate describes EPAs as units of professional work that can be entrusted to a trainee once sufficient competence has been demonstrated (ten Cate, 2005).
Examples of EPAs include conducting a patient consultation, managing a patient with acute symptoms, or presenting clinical findings during team rounds. These tasks integrate multiple competencies such as clinical reasoning, communication, and professionalism.
Because EPAs represent real clinical responsibilities, supervisors must observe how trainees perform them in practice. Evidence may come from direct observation, workplace based assessments, or structured evaluations of recorded clinical encounters.
Once a trainee consistently performs an EPA at the expected level, supervisors may grant greater autonomy. Over time, trainees accumulate entrustment decisions that demonstrate readiness for independent clinical practice.
The future of competency based medical education
Competency based medical education continues to evolve as training programs refine assessment systems and digital tools that support competency tracking.
Many institutions now integrate electronic portfolios and structured assessment platforms that collect evidence from multiple clinical encounters. These systems help programs monitor progression across competencies and identify areas where trainees need additional support.
Simulation based training also contributes to competency development. Simulation environments allow trainees to practice complex clinical scenarios and receive structured feedback before encountering similar situations in real patient care.
At the same time, educators continue to explore new methods for capturing authentic clinical performance. Technologies that support video recording, structured evaluation, and longitudinal feedback may play an increasingly important role in documenting competence.
As healthcare education becomes more outcome oriented, CBME will likely remain central to training physicians who can demonstrate their abilities in real clinical practice.