

Empathic Accuracy vs Empathy in Healthcare Training
Empathic accuracy and empathy are related, but they are not the same clinical skill. Empathy describes how a clinician connects with a patient’s experience. Empathic accuracy asks a sharper question: did the clinician correctly understand what the patient was thinking or feeling?
This distinction matters in healthcare training because a learner can sound caring and still misunderstand the patient. They may use a warm tone, nod at the right moments, and offer reassurance, yet miss the actual concern behind the patient’s words.
Therefore, empathic accuracy should be trained as an observable process: notice the cue, form a tentative interpretation, check it with the patient, and adjust when the patient clarifies. This connects directly with responding to emotional cues in healthcare.
Empathic accuracy vs empathy
| Concept | What it means | Clinical risk | Training focus |
|---|---|---|---|
| Empathy | Showing concern, warmth, and emotional engagement | The clinician may sound empathic but still misunderstand | Presence, acknowledgment, tone, and patient centered language |
| Empathic accuracy | Correctly interpreting what the patient feels, means, or worries about | The clinician may assume too much | Observation, interpretation, checking, and correction |
| Sympathy | Feeling sorry for the patient | The clinician may overidentify or lose clinical focus | Boundaries and professional support |
| Reassurance | Trying to reduce distress quickly | The clinician may close the emotion too early | Explore before reassuring |
Why clinicians misread patients
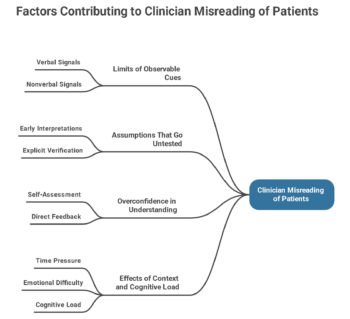
Clinicians misread patients because communication depends on inference. Patients often share emotional or social concerns through indirect clues rather than direct statements.
For example, a patient may say, “I live alone,” after hearing about discharge. The literal meaning is simple. However, the emotional meaning may involve fear, practical insecurity, or worry about coping at home.
Research on patient clues found that patients often introduced personal or emotional concerns indirectly during primary care and surgical visits. Yet clinicians missed many of these opportunities.
As a result, empathic accuracy should not depend on intuition alone. Students need to learn how to check their interpretation before moving on.
A practical model for empathic accuracy
Educators can train empathic accuracy with four steps.
| Step | What the learner does | Example phrase |
|---|---|---|
| Observe | Notice the cue without judging it | “The patient paused after I mentioned surgery.” |
| Infer | Make a tentative interpretation | “They may feel worried or unsure.” |
| Check | Ask the patient to confirm or correct | “I wonder if this feels worrying. Is that right?” |
| Adjust | Change the response based on the patient’s answer | “So the main concern is recovery time, not the procedure itself.” |
This model keeps empathy grounded. The learner does not need to guess perfectly. Instead, they need to stay curious and correctable.
Example 1: The patient says “I’m fine”
A student explains a diagnosis. The patient looks down, speaks quietly, and says, “I’m fine.” The student accepts the answer and continues with treatment instructions.
This may show empathy in style, but weak empathic accuracy. The learner noticed the words but did not check whether the patient’s tone and behavior matched them.
A stronger response would be: “You said you’re fine, but I noticed you went quiet there. What is going through your mind?”
This response avoids accusation. It also gives the patient room to confirm, deny, or clarify the learner’s interpretation.
Educators can use this example during emotional cue training, because it shows how accuracy depends on checking meaning, not only noticing emotion.
Example 2: The learner reassures too early
A patient says, “I’m scared this treatment will change my life.” The learner responds, “Don’t worry, we do this all the time.”
The response may come from kindness. However, the learner has not yet understood what the patient fears. The concern may involve pain, cost, fertility, family roles, work, or loss of independence.
A more accurate response would be: “That sounds like a big worry. What part of the treatment feels most life changing?”
This improves empathic accuracy because the learner stops guessing and invites the patient to define the concern.
In feedback, educators can ask: did the student reduce emotion, or did the student understand it?
Example 3: The clinician assumes agreement
A patient says, “Whatever you think is best.” The clinician may interpret this as trust. However, the patient may feel overwhelmed, unsure, or uncomfortable disagreeing.
Empathic accuracy requires checking the meaning of quick agreement. A useful response is: “I can give a medical recommendation, but I also want to understand what matters most to you.”
This connects empathic accuracy with shared decision making in healthcare. If the clinician misreads agreement, the decision may look shared while the patient remains passive.
For trainees, the skill is not only explaining options. It is also checking whether the patient has expressed a real preference.
How to assess empathic accuracy
Empathic accuracy needs more than a global comment such as “good empathy.” Educators should assess the sequence of behavior.
- Did the learner notice a verbal or nonverbal cue?
- Did the learner form a tentative interpretation?
- Did the learner check that interpretation?
- Did the learner adjust after the patient clarified?
- Did the care plan reflect the patient’s actual concern?
This approach fits communication skills assessment because it turns empathy into observable actions.
It also works well in OSCEs. Standardized patients can provide emotional cues, then reveal more only if the learner checks the cue properly.
How video helps train empathic accuracy
Video helps because learners often remember what they intended, not what they actually did. A recording gives the student, peer, and educator the same evidence.
During review, educators can pause a consultation and ask:
- What cue appeared here?
- What did the learner seem to infer?
- Did the learner check the interpretation?
- What did the patient do after the response?
- What could the learner try next time?
Research on video based feedback using real consultations supports video review as a way to strengthen self perception, peer feedback, patient centered reflection, and reflective practice.
For programs using video recording software for medicine, this creates a practical way to review accuracy, not just style.
Common mistakes when teaching empathic accuracy
The first mistake is treating empathic accuracy as mind reading. Students should not claim they know what the patient feels. They should check.
The second mistake is confusing warmth with understanding. A supportive tone matters, but it does not prove that the learner interpreted the concern correctly.
The third mistake is rewarding scripted empathy. Phrases such as “that must be hard” can help, but they become empty if the learner never explores what is hard.
The fourth mistake is ignoring the learner’s own emotions. Halpern argues that clinicians should not detach completely from emotion. Instead, they can use emotional awareness carefully to understand patients while maintaining professional judgment.
This connects with self awareness and self reflection, because learners need to notice their own reactions before they interpret the patient.
Final thoughts
Empathy helps clinicians connect. Empathic accuracy helps them understand correctly.
In healthcare training, both matter. However, educators should not assume that a caring response means the learner understood the patient. Students need to practise noticing cues, checking interpretations, and correcting assumptions.
When empathic accuracy becomes visible, feedback becomes more precise. Educators can stop saying “be more empathic” and start asking: “What did you think the patient meant, and how did you check?”
That question changes the training goal. It moves learners from performing empathy to understanding patients more accurately.
References
Suchman AL, Markakis K, Beckman HB, Frankel R. A Model of Empathic Communication in the Medical Interview. JAMA. 1997.
Levinson W, Gorawara Bhat R, Lamb J. A Study of Patient Clues and Physician Responses in Primary Care and Surgical Settings. JAMA. 2000.
Halpern J. From Detached Concern to Empathy. Oxford University Press. 2001.
Lim BT, Moriarty H, Huthwaite M. Being in role: A teaching innovation to enhance empathic communication skills. Medical Teacher. 2011.
Dohms MC, Collares CF, Tibério IC. Video based feedback using real consultations for a formative assessment in communication skills. BMC Medical Education. 2020.
Alves Nogueira AC, Melo C, Canavarro MC, Carona C. Emotion regulation in physician patient communication training. BJPsych Advances. 2025.